Are we ‘in the Suicide Prevention business’ or is it Suicide Maintenance?
A provocative title of course, partly to grab attention, but partly to make an extremely serious point. If we’re ‘in the suicide prevention business’, we should surely be doing all we can to get the numbers of suicides on a downward trend, towards zero? And if we’re not doing that, we’re effectively ‘in the suicide maintenance business’ aren’t we?!
The Government’s Suicide Prevention Strategy for England, 2023–2028
I started writing this article-which-has-turned-into-a-30,000-word-dissertation almost three months ago after the publication of the Government’s new 2023–2028 National Suicide Prevention Strategy for England (NSPS), which was released on Monday 11 September 2023, the day after World Suicide Prevention Day.
I thought I’d write a thorough review of the new National Strategy, although I then questioned whether it was worth the investment of my precious time because the 2023–2028 Strategy publication is a thin offering that doesn’t need much in-depth analysis to see through its low ambition and low likelihood of impact on the suicide numbers.
But then my deep-rooted principles spoke to me and I thought “it’s crucially important to have proper scrutiny and accountability”; and I decided to write a very detailed critique of the Government’s dreadful ‘Strategy’ for anyone who shares my concerns — also maybe as a wake up call for those sleepwalking through this tragedy-on-a-tragedy — and to explain why these national strategies and plans (in the UK and in other countries) always fall so woefully short of where we need to be on suicide prevention.
It also provided another opportunity for me to talk some more about key change dynamics, and tackling suicide prevention as one of the great transformational change challenges of our time…right up there with tackling climate change, because there’s so much we can do to stop preventable suicide deaths as well as to prevent extinction of our planet.
After 12 months’ delay in us getting the new National Strategy, including several of the regular meetings Steve Phillip and I have with DHSC, with us asking “any news on the new National Strategy?” only to be told “no, nothing to report…no scheduled publication date” and, in the absence of any open engagement or public consultation around the 2023–2028 NSPS, I thought a thorough analysis might be appreciated by some of those I work with. Indeed, a couple of Suicide Prevention Leads encouraged me to write it.
Please note this piece I’m writing here now — a critique from the personal and professional perspective of someone who thinks this National Strategy goes beyond the usual woeful low ambition by being shameful in some of its phrasing and framing and, in parts, potentially harmful — is in addition to the formal published response to the NSPS from The Jordan Legacy, which was published on Thursday 21 September 2023, after our meetings with some of the ‘key stakeholders’, including DHSC and some of those directly involved in pulling the new National Strategy together.
For the record, direct input from Steve and I into this National Strategy was limited to just a single opportunity via one online forum on ‘Targets and Measurement’ and, remarkably, the Government then chose to not even set a target for reduction of suicides —which many in our network (of people with lived experience) believe is ‘giving up’ on suicide prevention!
And, indeed, we’ve heard people in positions of power and influence actually saying “maybe we do need to think about shifting our focus from preventing suicides — accepting this 6000+ pa number — to helping people impacted by suicide”.
This is dangerous, defeatist thinking!
One of the best ways, if not the best way, to help people impacted by suicide is to get the suicide numbers down, towards zero, so these people can live with greater hope that 6,000+ suicides per year is not inevitable, not regarded as acceptable, indeed never ever regarded as acceptable!
Many of those impacted by suicide, like Steve and myself, make it a life mission to do what we can to minimise the number of suicides so, in this context, ‘focusing on helping people impacted by suicide’ actually means making every effort possible to prevent all preventable suicides, including preventing people bereaved by suicide from taking their own lives.
The formal response from The Jordan Legacy was written after very careful consideration of what we thought was a fair and reasonable perspective, with fair and reasonable criticism of this long-awaited-then-extremely-disappointing offering.
You can read The Jordan Legacy’s published response to the NSPS here:
In my own more detailed review below of the new National Suicide Prevention Strategy, I’ll go into more depth on some complex issues and nuanced points…and not hold back…so strap yourself in!
First, a quick summary, and a warning.
The 2023–2028 National Strategy Lacks Ambition, Targets, Money & Hope!
The Government’s new National Suicide Prevention Strategy is yet another low ambition offering which may in fact have set the bar at an even lower level than the previous Strategy, although it’s difficult to tell because of the Government’s decision to not even include a reduction target this time.
In the previous National Strategy and related plans, the Government set what most people, certainly most people with lived experience of suicide, regarded as a low ambition target of ‘10% reduction in 5 years’.
One of the main reasons why ‘10% reduction in 5 years’ is generally regarded as a low ambition target is that all the evidence we have, and all the advice we get from ‘experts’ like President of the International Association for Suicide Prevention (IASP), Professor Rory O’Connor from the University of Glasgow, is that “most suicides are preventable”.
Indeed Rory often says “all suicides are preventable right up until the last moment” although some think that’s a contentious statement, but all agree that “most suicides are preventable”.
So, everyone reasonably concludes, we should be trying to prevent most suicides, which translates into a target of, say, 50% reduction right?
For those not aware, this institutionalised low ambition has actually become known as a ‘syndrome’ among the global ‘Zero Suicide community’. It’s known as “The ‘10% reduction in 5 years’ problem”.
This was after the World Health Organisation (WHO) in its first global report on suicide prevention in 2014 (yes, that’s right, only in 2014 did we get a WHO report!) urged every country to set a target of ‘a minimum of 10% reduction in 5 years’ — note a MINIMUM of 10% reduction in 5 years — and only two countries in the world chose to aim higher than the recommended minimum target. Almost every country opted to ‘go low’ at precisely 10% reduction in 5 years, including England.
So, the previous NSPS for England ‘went low’ and adopted the target of ‘10% reduction in 5 years’ in a ‘forward plan’ within the NSPS that was supposed to deliver this reduction by 2020. [Spoiler alert: it didn’t!]
This is a key date, especially given Minister Maria Caulfield’s appearance on BBC Breakfast when the new NSPS was launched and she talked about ‘progress being halted by the pandemic’ because the inconvenient truth is the plan was to reduce the numbers of suicides by 10% by 2020, so we should have seen progress before the pandemic even emerged.
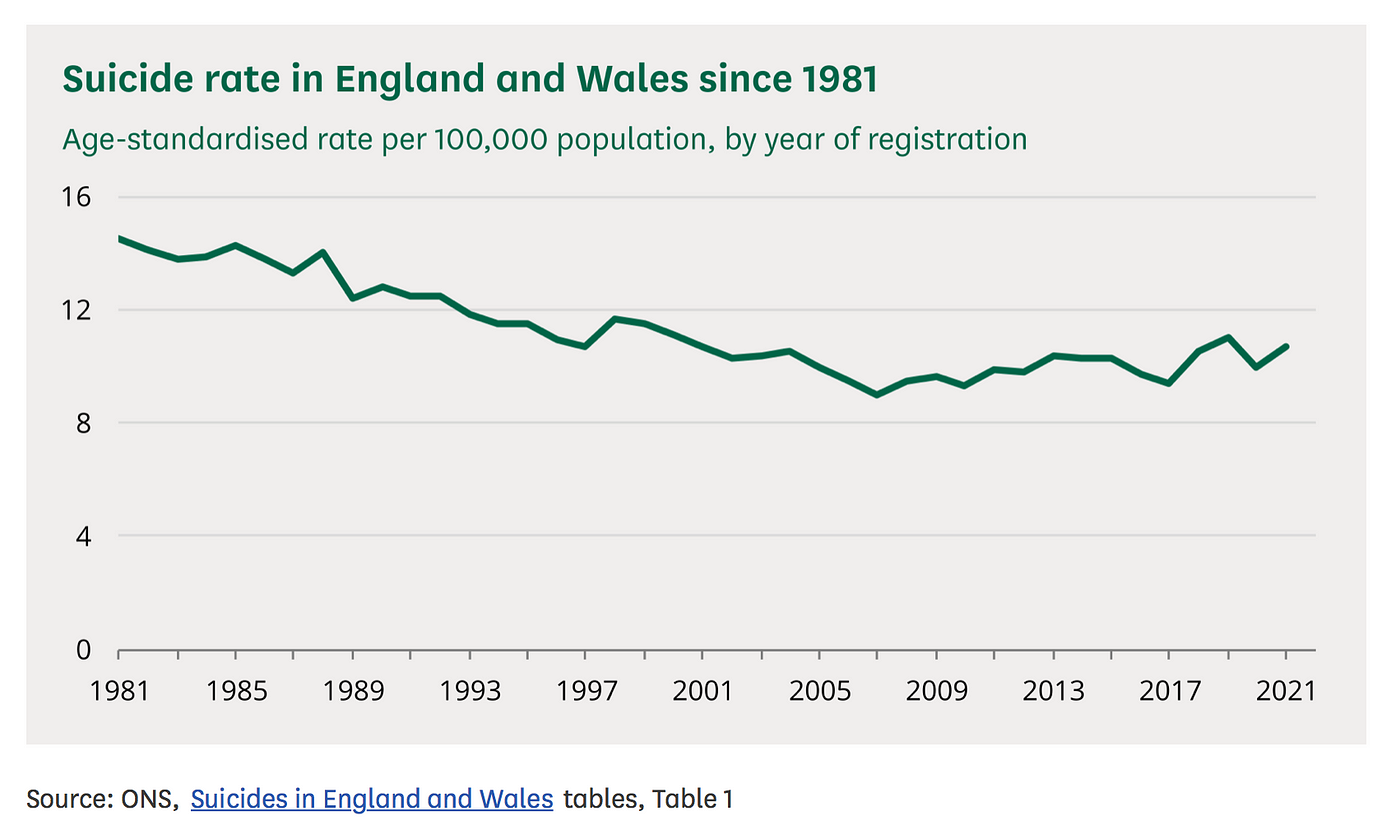
Let’s just look at that chart carefully, and study the actual numbers:
Yes, that’s right, the suicide rate went UP— and don’t be fooled by anyone telling you that we need to take into account that the burden of proof for Inquests changed from ‘beyond reasonable doubt’ to ‘balance of probabilities’ because that was only approved by the High Court in 2019.
So, the Government’s previous NSPS set the low ambition target of ‘10% reduction in 5 years’ and then failed to meet even such a low bar target.
And this new NSPS? Well, that’s a bit of a story, and not one with a happy ending because of the latest Strategy not having a target at all.
At the online forum that Steve Phillip and I were invited to, hosted by the National Suicide Prevention Alliance (NSPA) — the only formal invite we had to input into this NSPS remember, despite our extensive and intensive knowledge of what works in reducing the suicide numbers and having access to hundreds of people with lived experience of suicide in our network— we were asked to focus on the topic of “targets and measurement”.
There were some people putting forward a case for lower targets to “be realistic”, ie “if we can’t achieve a 10% reduction, why set a target higher than that?” — which is the ‘institutionalised low ambition’ syndrome in play again of course — and then some urging higher targets to “demonstrate ambition”.
Some of us from the ‘Zero Suicide Society community’ put forward a case for higher ambition targets like falls of 20%, 25%, 50% or more, to have the kind of ‘stretch targets’ that can drive the reductions in suicides we need.
And, fair to say, there were the usual arguments against. Some based on the ‘realism’ card again; and some based on misunderstandings about ‘Zero Suicide’ — which is a philosophy and framework for driving numbers down ‘towards zero’ with all the necessary cultural and structural change that requires, it’s not just a bald numerical target.
Some did argue a case for not having a target at all, which is an argument that Steve and I also heard in our action research interviews, but this argument rests on still having clear targets for all the component parts of strategies and plans, just not an overall target. High aspiration, stretching targets and accountability still have to be baked in somewhere or the National Strategy is just a piece of paper (or, these days, an online scroll).
Many of those in our action research project, especially those with lived experience of suicide, told us “not setting an overall target for reduction in the suicide numbers would be like ‘giving up’ really”; and we made that point in the NSPA forum — our sole opportunity for NSPS input remember.
NSPA helpfully published a summary of the discussions that took place at that forum, and passed it on to the National Suicide Prevention Advisory Group advising the Government on its new National Strategy.
And so, we now have the Government’s new National Suicide Prevention Strategy for England — which had plenty of time to consider all of these issues — and what did they decide?
They decided to have no target at all for the overall reduction in suicide numbers — that very action (or inaction!) that our lived experience community said would be “like giving up”!
The NSPS states its “overall ambitions” (can we really call them ‘ambitions’?) and limits its commitment to:
“reduce the suicide rate over the next 5 years — with initial reductions observed within half this time or sooner”
Not inspiring is it?! It reads like someone who’s had a terrible day at the races who’s in the bookies with their last £10 desperately trying to think of an each-way bet that’ll at least give them one win before they go home!
And, of course, money is a big part of this.
The Government’s new National Suicide Prevention Strategy has no new money in it and, with existing programmes scheduled to run out in 2024 and 2025, the NSPS is projected to have fewer resources in Years 3–5.
So, in summary, the NSPS lacks ambition, it lacks a target — making the next level of targets sitting underneath that even more crucial for action, progress & accountability — it lacks the necessary resources to have impact and, for many people (with lived experience), it looks like ‘giving up’.
In that sense, the National Strategy lacks hope, and all of us involved in suicide prevention know how crucial it is to maintain hope.
With a bit of a scattergun, braindumping approach in the way the document has been written, another analogy that keeps coming into my mind is that the 2023–2028 National Suicide Prevention Strategy (is it really a strategy?) is a bit like someone with no money, and probably little hope of having the money they need, publishing their shopping list!
The NSPS does have some good measures in it, and you’ll see in The Jordan Legacy’s fair and balanced review that we’ve highlighted the good (in most cases ‘good, but could do better, and go further and faster’) as well as the bad and the ugly! — but overall…well let’s just say reading the content now it’s published would have been a massive disappointment if our expectations weren’t so low to begin with.
These low expectations are based on previous low ambition National Strategies and the reasonable assumption we’ll get more of the same, along with the 12 months’ delay in publication; the lack of public engagement or consultation; the very limited involvement of people with lived experience; poor communication around the NSPS; the fact that, very unprofessionally and disrespectfully, most ‘announcements’ about what was going to be in the NSPS were in the form of posts on ‘X/Twitter’ from the lead government adviser, Professor Sir Louis Appleby; compounded by the political spin that accompanied the launch, overstating progress since 2012 and understating the problem we’re trying to solve here so, potentially, creating further barriers to progress in reducing the number of suicides.
Remember you can read the formal published response to the new NSPS from The Jordan Legacy — a joint statement from myself and Steve Phillip — on The Jordan Legacy website here:
What follows here is my personal review, reflections & recommendations.
And Here’s That Warning!
I mentioned earlier there’d be a summary and also a warning. So, after the summary above, here’s the warning below.
At the events I’ve attended since the publication of the new SP Strategy, and in my many day-to-day conversations and exchanges via online business & social media, from LinkedIn to Facebook, I’ve had many people say “Isn’t it great the new National Strategy has been released (often followed by ‘at last’)”.
I say to them “Have you read it?” and the answer almost always comes back “Er, no…well…er, no, not yet…er, not all of it…er not in depth”.
I also saw a post just after it was published saying “I’ll be taking a look at this over the next few days but there is hope” to which I replied “I’ll also be reading it, and analysing it, very thoroughly over the next few days…then I’ll let you know if there’s hope”.
We mustn’t make assumptions or let the political spin pass us by without proper scrutiny, transparency and accountability.
Our democracy depends on it and, in this case with it being the National SUICIDE PREVENTION Strategy, many human lives depend on it.
Please, please, please read the NSPS or, at the very least, scan the Strategy document and read The Jordan Legacy’s published response.
And I hope you’ll also read my critique below and the first 5 pages of the published National Suicide Prevention Strategy: including the Foreword from Minister Maria Caulfield MP; the Foreword from long-standing lead adviser to government on all matters suicide prevention, Professor Sir Louis Appleby (btw, in our action research project, some people referred to the National Suicide Prevention Strategy as “Professor Appleby’s Strategy” or just “Appleby’s Strategy” emphasising the degree of influence that a lead adviser can have!); and also please read the (3-page) Executive Summary.
There’s enough content in those first 5 pages to demonstrate the lack of ambition, the lack of commitment to getting the numbers of suicides on a downward trend, towards zero; and to highlight that, despite some positive measures, aligned to what people with lived experience, ie people who are ‘experts in their own experience’, and other ‘experts’ told us in our action research, some of the NSPS content can only be described as woeful… in places, shameful…and, in a couple of instances, potentially harmful.
And one further concern; a major concern.
Since the NSPS for England 2023–2028 was published, I’ve seen several posts on LinkedIn, and comments on social media, and even a couple of speeches from local Suicide Prevention Leads and leaders of prominent national charities saying “we need to look at how we can implement the Government’s National Strategy”.
No we don’t! It’s not our job to implement the Government’s Strategy — on suicide prevention or anything else for that matter!
It’s our role to find ways of getting the suicide numbers on a long-term downward trend, towards zero. Governments can help us achieve this goal or frustrate us in achieving this goal. In recent history, it’s been the latter.
It’s the role of local Suicide Prevention Leads to reduce suicides in their area. If drawing from the National Strategy or working with the Government — as genuine collaborative partners with shared goals — helps to get the numbers down, then that’s what we’ll do, that’s what we should do. If not, we won’t; we shouldn’t; we should challenge appropriately.
If, like me and many others, you think the Government’s Suicide Prevention Strategy is woefully low on ambition, why would you want to help them implement their low ambition strategy?
Work with them to get them to aspire higher for sure, but not conspire in low ambition. As I’ve found myself saying a lot in these past few weeks “If you get into bed with low ambition, you tend to get infected with low ambition”!
The Suicide Numbers are Unacceptably High and Needlessly High!
In my suicide prevention work, and in analysing a document like the new NSPS, I wear various professional hats, including Research Fellow analysing the data and dynamics; experienced public policy analyst; change coach and consultant with 40 years’ experience working on systems change and transformational change programmes; and counsellor working in mental health & suicide prevention at one-to-one and small group level.
I also have my own lived experience, my own exposure to suicide, including losing many people to suicide — the first as long ago as 1980, the most recent being losing a family member in August 2020 — and I have my own tortured experience of debilitating depression with anxiety and many ‘complications’, which constantly reminds me that suicide is “not just a mental health issue”, a point that’s crucial to understand and act upon if we’re to get the suicide numbers moving downwards, towards zero.
I ‘think about’ and ‘feel about’ all of the above whenever I look at this chart below which is the chart MPs go to, or should go to if they haven’t seen it, in the House of Commons Library report on suicide rates.
It’s also the chart that Ministers and their advisers often ‘spin’ as showing a healthy picture of significant reduction in the suicide rate since 1981, without making it clear that reduction was in the period 1981 to 2007, with no reduction since 2007:
Also, in the debate around The LEARN Network’s petition for a statutory duty of care for students in higher education, one MP described the recent suicide figures as “mercifully low”!
For anyone who’s lost a loved one to suicide or who’s almost lost their own life and managed to survive a suicide attempt, and for all of those like myself, Steve Phillip and The Jordan Legacy advocating and campaigning for a ‘Zero Suicide Society’, these suicide numbers are not “mercifully low”, they’re unacceptably high!
And they’re needlessly high because all the evidence tells us that most suicides are preventable. We need ‘the will’. We have ‘the way’.
IASP President, Professor Rory O’Connor, told us “we know what works in preventing suicides, we’re just not good in putting this knowledge into practice”.
People with lived experience know ‘what works’ or what will work.
The Zero Suicide Society Transformation Programme
This is why we must listen to and learn from diverse lived experience voices — and go ‘wide and deep’ in our listening.
And it’s why the Zero Suicide Society Transformation Model is built on a foundation stone of listening to and learning from people with lived experience, as well as involving all the other key stakeholders who are part of the solution, because we know that ‘Involvement = Commitment’:

If you want to know more about the Zero Suicide Society Vision and Transformation Models, Frameworks and Programmes, including the Building Blocks/Jigsaw Picture Puzzle model illustrated above, you can read our (2nd Edition) Report ‘Moving Towards a Zero Suicide Society’ via this link:
Suicide Prevention as a Transformational Change Challenge
The report ‘Moving Towards a Zero Suicide Society’, which I co-authored with Steve Phillip, also highlights The 3 Key Dynamics of Change model that I’ve used in my transformational change consulting and coaching work for more than 30 years, and which I focus on in my lectures at business schools, and which I’ve applied to both our Zero Suicide Society model and the Government’s National Strategy for England 2023–2028. It’s quite a contrast!
There’s an explainer piece on this transformational change model here:
Essentially, suicide prevention is a transformational change challenge. Indeed, one of the great transformational change challenges of our time.
That makes it a rather scary prospect for many — and some have clearly ‘given up’ or ‘buried their heads in the sand’ — but others, especially those who work in transformational change being exposed to ‘the suicide problem’ for the first time, see it as a positive challenge we need to rise to, and an opportunity to show what we can do, especially without the polarising politics of other great challenges of our time like climate action.
In our action research and analysis, we applied The 3 Key Dynamics of Change model to our inputs and outputs and it passed the tests, always with room for improvement of course.
To effect transformational change, we need a powerful Push effect moving us away from our active dissatisfaction with the current state.
The report, and everything we do as part of the Zero Suicide Society Programme every day, makes it clear we’re deeply dissatisfied with the status quo with 6000+ preventable deaths by suicide in the UK, and 5,000+ preventable suicide deaths in England, each year for the past 15 years, with no reduction in those numbers over that long period.
It’s a problem that’s clearly not improving and without the capacity to improve when, for example, the number of children on NHS Child and Adolescent Mental Health Services’ waiting lists exceeded 1 million in January 2023 for the first time, and where adults having thoughts of suicide are being put on a 6 months’ waiting list for NHS Mental Health Services!
Push? We desperately need urgent Push, urgent action!
To effect transformational change, we also need a powerful Pull effect, motivating us to move towards a compelling future vision that’s achievable and therefore inspiring, energising, and a source of hope.
The Zero Suicide Society vision — a highly practical vision and a realistically achievable future desired state, not a utopian dream — provides this necessary Pull effect.
And, last but not least, transformational change needs a powerful Engagement and Involvement effect. Those who need to be part of the change must be involved in that change — Involvement = Commitment!
Those who have ‘the answers’ must be engaged and involved. In the case of suicide prevention, we know that people with lived experience of suicide have ‘the answers’ and we must learn from them, as well as listening to anyone widely regarded as an ‘expert’ in the field — avoiding self-appointed ‘experts’! — and anyone who potentially has solutions, including evidence-based ideas or ideas that may need us to search for new evidence.
We constantly strive to have wide and deep engagement and involvement.
We do pretty well — certainly for a tiny VCSE organisation which relies purely on donations for its income — but with the perspective and humility to accept that we’re not doing enough and we can do much more.
We’re about to launch a new project which will create ‘a deliberative and participative democracy map for the suicide prevention landscape’ which will show what more needs to be done on ‘lived experience involvement and engagement’ and how we can do it.
We plan to make this a collaborative exercise, partly because ‘technically’ this makes sense, and partly because it will be important symbolically — a wide and deep engagement about wide and deep engagement!
The NSPS 2023–2028 is not a Transformational Change Strategy!
We applied these same three tests to the Government’s new National Strategy for England — NSPS 2023–2028 — and on Push, Pull, Involve, the report card is ‘Fail, Fail, Inadequate’.
To be fair, no-one gets above ‘Inadequate’ for involving and engaging stakeholders, including specifically involving and engaging people with lived or living experiences of suicide, as we all have so far to go here.
All able to comment felt that lived experience involvement in developing the new NSPS was much improved on previous National Strategies — although several people recounted how the process for developing the Government’s first National Strategy in 2012 involved three people with lived experience so not hard to top that! — but it’s crucial for our change dynamics to accept that what we’ve all done to date is still Inadequate.
It’s definitely a big Fail on Pull as there’s no compelling vision mapped out in the NSPS 2023–2028, no real vision at all in fact, and many people have commented on this to us, often praising our report ‘Moving Towards a Zero Suicide Society’ for providing that vision as a much-needed source of hope and inspiration, as well as providing a practical road map.
And it’s a huge Fail on Push, because NSPS 2023–2028 and the subsequent communications around it, including the launch on 11 September, has appeared to play down the problem and talk up any evidence of progress in what is, at best, misunderstanding the crucial role dissatisfaction with the status quo plays in change dynamics and, at worst, the kind of political spin that causes so much unnecessary pain in our society and our democracy, which needs to be fed by honesty, transparency and accountability but is so often given the very opposite meal.
Communications for Change or for Inertia?
In our report ‘Moving Towards a Zero Suicide Society’ Second Edition, published on 28 September, two weeks after the Government released its new National Strategy, we highlighted the incongruence between what Mental Health Minister Maria Caulfield MP was saying and the actual evidence:

As part of the Minister’s media rounds on publication of the NSPS for 2023–2028, when asked by the BBC’s Jon Kay why it’s taken so long since 2012 to publish this new Strategy, with many lives being lost in this time, the Minister replied:
“Well, it’s really important to note the progress that’s been made during that time. We saw a 20% reduction in the number of suicides compared to, say, two decades ago…so it’s just before the pandemic that progress began to plateau so we haven’t seen a huge increase in the numbers but we haven’t seen a reduction either”.
Now we can be generous and say the Minister just got a bit flustered in the studio and a bit confused with the data, but let’s pick this statement apart.
Jon Kay was asking why there’s been no progress, in reducing suicide rates, since 2012, as he was aware of the ‘flat line’ since 2012.
The Minister did not acknowledge the lack of progress in terms of no reduction in the overall number of suicides since 2012 and, in direct contradiction, tried to imply there’d been progress.
She had two goes at it, in fact.
The first was implying there’d been a 20% reduction in suicides in the period since 2012 compared with the previous two decades. Not true of course, as the chart shows very clearly. The reduction came long before 2012, long before the first published NSPS was introduced in 2012.
The second go was implying progress between 2012 and 2019/20 with that progress ‘being halted by the pandemic’. Again, the chart shows this is not an evidence-based claim.
Was this mischievous political spin or simply a confused response under pressure? I’ll leave you to decide!
At the very end of her response, the Minister finally acknowledges there’s been no reduction in the numbers but her implication in her response as a whole is that there’d been a reduction 2012–2019/20 — which there wasn’t — and then no reduction since the pandemic reached our shores.
And to complete her confusion or obfuscation — again, you choose! — the Minister threw in “we haven’t seen a huge increase in the numbers” which also gives people the impression that everything might be rosy in the garden, and an attempt to reassure with there being no ‘huge increase’.
It’s often said that ‘the first step to solving a problem is accepting there’s a problem to be solved’. In all our communications at The Jordan Legacy, we consciously and very deliberately refer to “the unacceptably high level of suicide deaths” because 6000+ deaths each year in the UK, or 5000+ each year in England, is an unacceptably high number of suicide deaths.
We refer to “the needlessly high level of suicide deaths” because most suicides are preventable, and we know there are so many practical actions we can take to get the numbers on a downward trend, towards zero.
And we constantly highlight the ‘flat line’ in the graph, ie the fact that the suicide numbers in UK/England & Wales/England have not fallen for the past 15 years. We’ll have to start saying 16 years now we have 2022 data!
Regularly and highly visibly showing this graph highlighting the ‘flat line’ is the simplest way of highlighting the problem we’re trying to solve; it spurs on those who are already trying to get the line on a downward trend — although it can be dispiriting to see ‘no change’ year after year — and, importantly, it activates others who previously haven’t been involved in suicide prevention and not been aware there’s a problem to solve.
To get the change we need, we must frequently and prominently communicate that the suicide numbers are unacceptably high, needlessly high, and not coming down, with no reduction for these past 15 years. As described earlier, this is our important Push change dynamic.
What we often get though, very sadly and dangerously — at worst, putting lives at risk or in danger — is academics & other data commentators saying the current suicide numbers are “relatively low”, which is factually correct when comparing current suicide rates to, say, the 1980s, but extremely unhelpful and even damaging from a change dynamics perspective…
..and in that one case already highlighted earlier, by an MP standing up in parliament and describing the suicide numbers as “mercifully low”!
For the record, the MP in question was Paul Blomfield (Sheffield Central), and he made some good points, eg about the education system taking the strain due to NHS Mental Health Services being unable to cope, and he made some compassionate and supportive comments, including most importantly in my view “even one suicide is one too many” and — quoting Ged Flynn from PAPYRUS — “suicide is very much a preventable death” but, in opposing a statutory duty of care for universities, he also ‘framed the problem’ by saying the overall suicide numbers are “mercifully low” and “much lower among students…than among the population as a whole”…
…which, sadly, cancels out his positive comments and are part of what is a common (conscious or sub-conscious) narrative, among MPs and other people in positions of power and influence, that suicide rates are low and therefore not a big problem to be solved nor an issue to be prioritised.
As people who care about human life, as people who care passionately about reducing the numbers of suicides, as people who know there are practical actions we can take to get those suicide numbers on a downward trend, towards zero, as people who believe that with the right ‘will’ and the right ‘way’ we’re capable of halving the numbers of suicides within the next 5–10 years, and as people with lived or living experiences of suicide, including losing loved ones to suicide…we should never, ever describe the current suicide numbers as “mercifully low” or “reassuringly low” as I’ve heard another MP say!
NSPS 2023–2028: a Change & Action Dynamics Analysis Critique
(inc Forewords that are not taking us Forward!)
In the context of my own personal goal, my own primary goal for the remainder of my life and career, being to reduce the numbers of suicides in the UK and get them on a downward trend, towards zero, I’ll now provide a very detailed critique of the Government’s new National Suicide Prevention Strategy to illustrate the lack of help and the potential harm within this document.
It’s crucial that we challenge it, question it, pick it apart…and devise our own local and targeted strategies and action plans that we think will significantly reduce the numbers of suicides — the micro ‘Zero Suicide Plans’ that will add up to a ‘macro zero’ — and draw from the NSPS 2023–2028 as just one source (not the source) for our strategies and plans.
Apart from anything else, let’s have some self-respect, and empower ourselves to act as we believe we should act to get the change we want to bring about, not kowtow to the Government, especially one that appears to have no commitment to suicide prevention or which has run out of ideas for how to bring the numbers down, or both.
Where the Government’s strategies and plans are aligned with ours, helpful and not harmful, of course we’ll fully collaborate.
Even then, we need to make sure it’s true collaboration not a top-down, hierarchical misuse or abuse of power, status or influence. We must be partners, and all consider ourselves to be partners, tackling a complex, multi-faceted problem that the evidence clearly shows no-one person or organisation, not the Government nor its advisers, have ‘the solution’ to. Fundamentally, we need respect and we need humility.
A Word from the Minister
In the opening passage from NSPS 2023–2028 (see screenshot below ) it’s good that the Minister — our latest Minister through the revolving door of the mental health and suicide prevention portfolios! — acknowledges the devastating impact every suicide has.
This is not only the appropriate human response, and response we should expect from the Minister, it’s an essential component part of our Push change dynamic to get the numbers down.
The Minister then says she is/her Govt is “committed to reducing the number of lives lost to suicide” which I’d like to think is the case but the rest of the document, and her media interviews, cast doubt on this commitment.
Having no target at all for suicide reduction does look like ‘giving up’ on any aspirations to significantly reduce the suicide numbers, and not committing any new resources doesn’t breed confidence.
I’m discounting the £10 million DHSC VCSE Suicide Prevention Grant Fund, highlighted so prominently at the beginning of the NSPS document and featuring so strongly in the Minister’s public responses when asked about funding behind the National Strategy, because £10 million is a drop in the ocean when we’re talking about the funding needed to ‘tackle the mental health crisis’ and get the suicide numbers on a downward trend ‘to their lowest level ever’ as many have urged, including Samaritans.
Hopefully, that VCSE SP Fund will not only provide some useful prop-up funding for VCSEs doing really valuable work — the Fund will be covering operational costs for many existing activities with some development of existing and new activities — but it will also fund innovation, and new ideas, that can potentially be transformative.
[Postscript: I put in a submission on behalf of The Jordan Legacy for funds to demonstrate implementation of the Zero Suicide Society Transformation Model & Programme, along with a crucial ‘Join the Dots’ initiative linking together otherwise disconnected parts of the system, and a scoping study to develop a prototype support centre transferable across the country; with all parts being transformational change proposals, not trying to prop up the status quo or stick a finger in the dyke! But we got a ‘no’ from DHSC].

The most worrying aspect of the Minister’s words — both above in the NSPS document and also in her media interviews — is the emphasis she places on ‘progress’ since 2012.
Now where there really is progress, it’s crucially important to highlight it and to suitably ‘celebrate’ it, although ‘celebrating’ progress in suicide prevention is a very difficult thing to do because even if we’d halved the numbers of suicides and felt like we should be having a party to mark this great achievement that would still mean thousands of people losing their lives each year and individuals out there in pain at losing their loved ones who wouldn’t be impressed by an overt celebration of fewer deaths while we still have so many preventable tragedies.
But, privately, in the right kinds of environments, using the most appropriate and sensitive language, it’s important for our change dynamics to recognise progress where it truly is progress as this spurs us on to go further, and perhaps faster.
For example, the NSPS 2023–2028 refers to a fall in the number of in-patient suicides by 35% between 2010–2020 so this is definitely worthy of recognition, although tempered with two qualifications.
Firstly, a 35% reduction is still not enough of course and we should have high aspirations for reducing the number of suicides for those ‘within the system’, ie where we know who these people are, in contrast to those in the community who ‘suddenly’ end their lives ‘without warning’; we know they’re at risk or in danger; we know what support they need; and we have the potential to provide the treatment, care and support they need, including on discharge — and continually trying to improve community-based services that reduce the numbers needing to enter ‘the mental health system’ — to keep more of these people ‘alive and well’.
Secondly, note the timeline for this reduction, 2010–2020, and the timeline for the Government’s first, publicly announced, NSPS from 2012. Any new strategy takes some time to have an effect, so the Strategy introduced in 2012 would have started having some impacts from 2013–2014 and, where actions involved systems changes, perhaps from 2015–2017. We must take care not to attribute too much of a reduction in in-patient suicide numbers 2010–2020 to a new Strategy announced in September 2012!
The Minister in her foreword saying “In developing this strategy, we have set out how we can build on the progress made over the past 11 years…” is not unsurprising positioning for a politician who’s a member of the party that’s formed Government for the past 11 years but it becomes a problem in terms of change dynamics when the (political) narrative is centred around ‘progress’ and the suicide numbers are not going down.
Let’s just look at that ‘flat line chart’ one more time, and reflect:
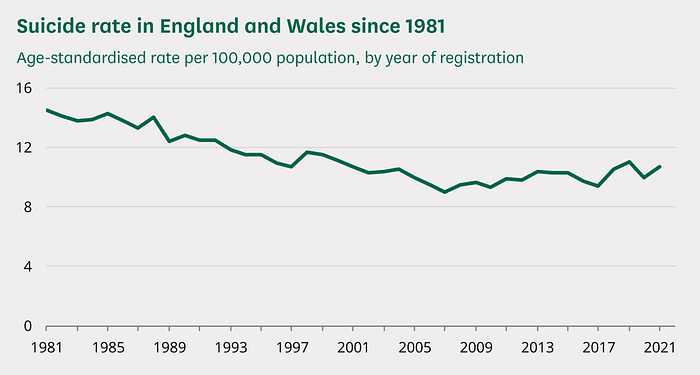
It’s not ‘progress since 2012’ is it?!
A Word from The Government’s Lead Adviser
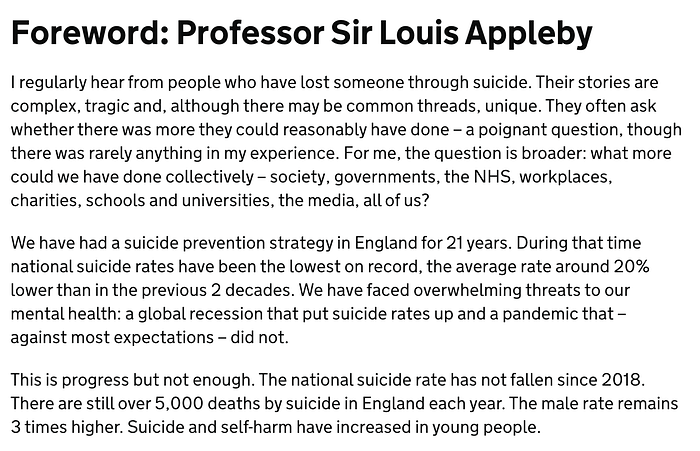
Following the Minister’s opening comments in NSPS 2023–2028, we have the Foreword from the lead adviser to the Government on suicide prevention, Professor Sir Louis Appleby. Prof Appleby has been the lead adviser on suicide prevention for many years, including for previous national strategies and plans.
As far as most people are concerned, the first National Strategy was that released in 2012 because that was the first published document that was generally known to be “the National Suicide Prevention Strategy” — and, in her media rounds on 11 September, the Minister referred to the 2012 document as “the first National Strategy”…
…although Professor Appleby says in his Foreword “We have had a suicide prevention strategy in England for 21 years”, ie going back to 2002, so we might want to take this into account in our analysis or just focus on the period since 2012 when the whole process has had some semblance of transparency and public accountability..
…although the lack of transparency and accountability around the National Strategy is a common criticism, including most public communication around the National Strategy being in the form of Prof Appleby’s Tweets.
Professor Appleby’s opening paragraph (see screenshot below) displays humanity and is a good summary of the situation we face. Individuals experiencing loss and pain ask what they could have done when there is often nothing (more) they could have done but there’s a lot more ‘the system’ could do to prevent future losses, future pain, future suffering.
His second paragraph is rather disturbing though, from a change dynamics perspective as well as from the human perspective of someone whose life has been touched by suicide on multiple occasions.
As just noted, he says “We have had a suicide prevention strategy in England for 21 years” and then continues “During that time, national suicide rates have been the lowest on record, the average rate around 20% lower than in the previous 2 decades”.
This is dangerously close territory to the MP who described current suicide rates as “mercifully low”!
For our Push dynamic, we need to emphasise that the current level of suicides, and the level they’ve been at for the past 11 years, and most of the past 21 years, is ‘unacceptably and needlessly high’. Without that clear expression of dissatisfaction with the status quo, we risk fuelling the inertia dynamic that is saying ‘no problem to be solved’ and holding back progress.
As soon as we start framing the numbers as ‘relatively low historically’ or ‘the lowest on record’, even if this is factually correct, we’re weakening our Push dynamic and encouraging others to think there’s not a problem to be solved here, including those MPs who might be tempted to use damaging lines like ‘reassuringly low’ or ‘mercifully low’.
Given that it doesn’t help us in achieving our goal of reducing the numbers of suicides and could actually hinder us, some would argue that this point about suicide rates being “the lowest on record” for the past 21 years should not appear in this Strategy document at all, certainly not so prominently in the Foreword by the Government’s lead adviser.
As with all so-called ‘evidence-based statements’, we also need to take care with our use and interpretation. The implication here — and in Professor Appleby’s public posts on this particular point — appears to be that having National Suicide Prevention Strategies has helped to keep suicide rates low.
This is a contestable claim and, again, it raises questions from a change dynamics perspective. It’s also at the heart of the low aspirations baked in to the latest NSPS for 2023–2028.
If we’re approaching this ‘problem’ — and talking up the fact it is a problem, not playing it down as the numbers being ‘relatively low’ or there being ‘huge progress since 2012’ — as needing to get the suicide numbers on a downward trend (some of us would add ‘towards zero’ but most would certainly agree the aspiration is a ‘downward trend’), then our ambition should be clearly stated as this, and our language should be geared to not just clarifying this but helping us achieve our goal and not hinder us.
The ‘fact’ that, for the past 21 years, “national suicide rates have been the lowest on record, the average rate around 20% lower than in the previous 2 decades” is not relevant and not a helpful ‘fact’ to highlight when trying to get the suicide rates on a long-term downward trend (towards zero).
Let’s look at that chart again:
The chart shows suicide rates on a downward trend from 1981 until 2007 and then what we often refer to as the ‘flat line’ since then.
Although we use the term ‘flat line’, suicide rates have actually gone up, even allowing for the burden of proof at Inquests being changed (from ‘beyond reasonable doubt’ to ‘balance of probabilities’) since 2019.
We tend to use the term ‘flat line’ because our aspiration is to get the suicide numbers on a long-term downward trend, towards zero, and what we’re doing when interpreting this key graph is saying ‘the downward trend from 1981 to 2007 should have continued but it’s basically flat-lined since’.
If we try to argue that suicide rates have gone up since 2007, the argument gets technical and nuanced and it changes the focus from trying to get the numbers down to arguing about the data, which benefits no-one except the ‘data nerds’ who love arguing about data!
If we frame it as ‘no reduction for the past 15 years’, that’s both factually correct and helpful as a change dynamic.
The phrase ‘flat-lined’ is a shorthand we may or may not wish to use, but the data clearly shows ‘no reduction for the past 15 years’ so that’s where our focus should be, along with getting that trend line going down.
According to the Minister, the first National Suicide Prevention Strategy for England was introduced (at least published) in 2012. The data tells us there’s been no reduction in suicide rates since then, with a case for arguing that rates have gone up since 2012. This is why the Minister’s emphasis on ‘progress since 2012’ is so problematic.
According to Professor Appleby, “we have had a suicide prevention strategy in England for 21 years”, ie since 2002. The data tells us that in that period there was a continuation of the historic fall in suicide rates 2002–7, and then a rise 2007–2013, and then it’s basically remained flat since 2013.
Based on this evidence, it’s clear the introduction of National Strategies — whether from 2002 or 2012 — has NOT led to a reduction in suicide rates.
And the main argument for investing in National Strategies — in England and in other countries that have introduced National Strategies, including Australia where I was more directly involved — is to get the suicide numbers on a long-term downward trend (towards zero).
In this sense, let’s not be afraid to say it, the National Strategies for England have failed in this fundamental aim.
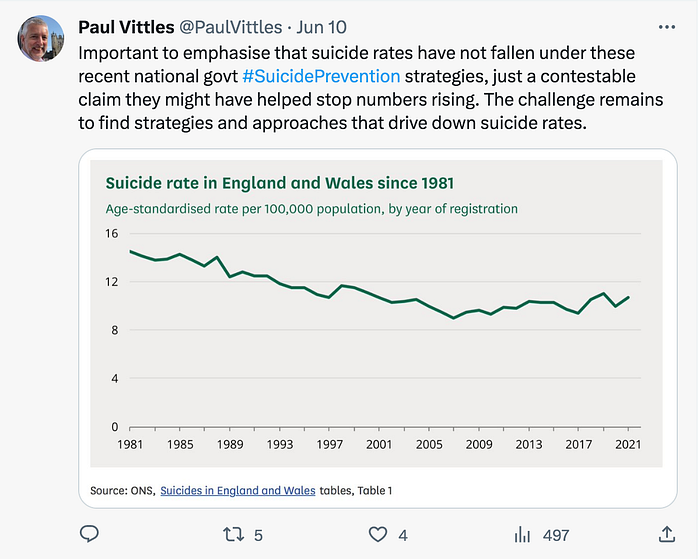
Let’s now return to the contestable claim that having these National Strategies have been a success because they’ve ‘stopped the numbers rising further’ or as Professor Appleby puts it in his Foreword “We have faced overwhelming threats to our mental health: a global recession that put suicide rates up and a pandemic that — against most expectations — did not”.
As I say, this is a ‘contestable claim’ so we’re not going to get a consensus view but we do need to ask ourselves which narrative we’re buying into.
In the period 1981–2007, when suicide rates were on the kind of downward trend we want to see revived right now, there were two deep recessions in England, two very different types of recession including the early 1980s where there were massive job losses in the old industrial parts of the country and suicides increased in these areas, as I personally experienced, and then the early 1990s where the job losses were much more spread across the country and across demographic and socio-economic groups including significant increases in ‘white collar’ unemployment, again placing upward pressure on suicide rates.
And yet, despite these two deep, biting recessions, the overall suicide rates in England were coming down, for a whole host of reasons. It’s rather disingenuous, therefore, to argue that National Strategies since 2002 or 2012 have been unable to keep suicide rates on a downward trend because of the recession caused by the global financial crisis in 2008–2009.
Of course, the global COVID pandemic was an exceptional event, but this hit us with real impact when we had the first Lockdown from March 2020. Much evidence, which Professor Appleby himself has highlighted, has shown that this period with these Lockdowns did not lead to an increase in suicide rates, although there may still be some delayed impacts to come, eg businesses that depleted all reserves during that period that have survived until now but may not make it through the next 5 years.
Suicide rates were not going down 2012 to March 2020 so we can’t blame the pandemic for our failure to reduce suicide rates during this period.
Another disturbing comment from the Minister when launching the new NSPS 2023–2028 on BBC Breakfast was about ‘making progress until the pandemic’. Let me just remind you of her exact words.
Asked by the BBC’s Jon Kay why it’s taken so long since 2012 to publish this new Strategy, the Minister replied “Well, it’s really important to note the progress that’s been made during that time. We saw a 20% reduction in the number of suicides compared to, say, two decades ago…so it’s just before the pandemic that progress began to plateau so we haven’t seen a huge increase in the numbers but we haven’t seen a reduction either”.
As I’ve already highlighted, the Minister’s statement implies a 20% reduction in suicides between 2012 and 2019/20 compared with ‘two decades ago’, which wasn’t the case; and that this progress was ‘only halted by the pandemic’ — not true because there was no reduction in this period, the (20%) reduction came prior to 2012.
So, we’ve got the Minister suggesting we’ve reduced the suicide numbers since 2012, which we haven’t, implying a 20% reduction which is clearly not the case, and Prof Appleby suggesting the numbers of suicides could have been even higher in the period since 2012 due to the upward pressures of recession, despite the fact we had deep recessions in the early 1980s and again in the early 1990s when suicide numbers were on a downward trend.
And, again trying to be generous, maybe the Minister got a bit confused with Prof Appleby’s text in this Foreword when he says, of the period 2002 to the present, “during that time, national suicide rates have been the lowest on record, the average rate around 20% lower than in the previous 2 decades”?
As the chart shows, the suicide rates may have been, on average, 20% lower 2002–2021 compared with the 2 decades prior to that but this is not due to the existence of National Strategies because the bulk of that 20% fall was pre-2002 and all of it was pre-2012.
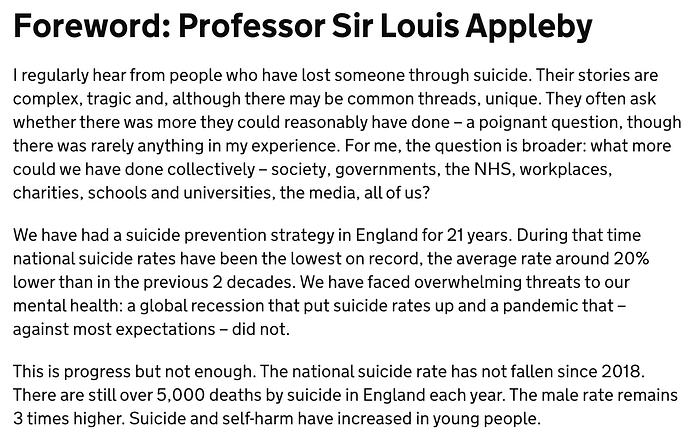
In his Foreword, Professor Appleby then says “This is progress but not enough” and, thankfully, goes on to give us a bit of a Push dynamic with “There are still over 5,000 deaths by suicide in England each year” and “Suicide and self-harm have increased in young people”.
But, again, whether there’s actually been ‘progress’ is a moot point.
With no reduction in the overall numbers of suicides, many of us would argue there’s not been progress, so it’s not a case of ‘not enough progress’, it’s a case of ‘no progress’.
And Professor Appleby also adds the line “The national suicide rate has not fallen since 2018”. That is definitely true but it’s also true that the national suicide rate hasn’t been on a downward trend since 2007.
Now you can say ‘it went up a bit, then down a bit, then up a bit so, technically speaking, it did go down a bit before going up again after 2017 so again, technically speaking, ‘it hasn’t gone down since 2018'.
But for those of us wanting to get the suicide numbers on a downward trend, towards zero, and embrace that Push change dynamic, we would look at that data and say “the suicide rate hasn’t gone down for the past 15 years” or “the suicide numbers have remained at an unacceptably high level of 5,000+ preventable deaths for each of the past 15 years”.
Both of these forms of words and numbers would not only be evidence-based, factually correct statements, but also emphasise the problem we’re trying to solve here, the priority and urgency of the problem we’re trying to solve here, and the desperate need to do something to prevent us losing another 5,000 people next year and the year after that and the year after that and the year after that…
Just saying “the national suicide rate hasn’t fallen since 2018” is another example, consciously or subconsciously, of downplaying the problem here. For the vast majority of people who don’t know the details of the data, nor these nuances of interpretation, ‘no reduction since 2018’ sounds so much more palatable than ‘no reduction for the past 15 years’. It encourages disengagement. It encourages inaction. The very opposite of what we need!
To be fair, ‘no reduction since 2018’ is still informing readers of the document that there’s been no ‘success’ for 5 years, so that has some benefit, but ‘no reduction for 15 years’ emphasises the scale of the problem much much better.
Some might argue ‘no reduction for 15 years’ might encourage people to think there’s no scope for further reduction but that’s part of the change challenge — emphasising the ambition, the vision, what practical steps we can take, giving confidence that we can get the numbers on a long-term trend down, towards zero. Sadly, NSPS 2023–2028 fails to do this.
Professor Appleby has a feared reputation, especially among campaigners trying to make their case using data, for being a stickler for accuracy in data, interpretation of data, and presentation of data, so I’m sure he wouldn’t want anyone to misinterpret statements like “During 20yrs of current strategy, suicide rates have been lower than at any previous time”:
As I replied at the time:
NSPS ‘Why We Need a New Suicide Prevention Strategy’
(inc why we need honesty, transparency, accountability, and ambition!)
Well that was a lot of time spent on the two Forewords, but they’re important. It’s the Minister with portfolio responsibility for suicide prevention and the Government’s lead adviser on suicide prevention for the period covered by these National Strategies framing the latest Strategy for the consumption of readers — many of whom will just read the two Forewords and the Executive Summary — and also framing the public conversation around the NSPS 2023–2028, so worth that investment of time.
The next section of the NSPS document — screenshot below — covers why we need a new national suicide prevention strategy.
Once again, it begins with the ‘considerable progress since 2012’ narrative. This of course is not progress in reducing the suicide numbers. It’s ‘progress’ in terms of ‘implementing priorities’. And, as we’ve been highlighting for some time, the focus on priorities — ‘The Priority Trap’ — is itself problematic, itself a barrier to reducing the suicide numbers. So ‘progress’ in ‘implementing priorities’ is not really progress at all!
And “Local authorities, NHS organisations, and suicide prevention organisations have aligned their suicide prevention activities with the national strategy” is not necessarily progress either, as there are two traps here — ‘The Priority Trap’, ie having winners and losers in a zero sum game where the overall suicide numbers don’t go down, and ‘The Top Down Trap’ where numbers don’t fall because local plans are driven by priorities in national plans rather than being shaped around local priorities.
The NHS is probably an exception because of its inherent top-down structure and culture and ‘sameness’ at its core, ie trying to provide the same nature and standard of care everywhere in the country.
It’s possible, and often desirable, to drive change from the top in the NHS — as long as local innovation is also encouraged as this can drive changes that can then be shared across the system, not just be ‘thought of at the top’.
The 35% fall in suicides among those in NHS Mental Health in-patient settings between 2010 and 2020, some of which may have been fostered by the National Strategy launched in 2012, is the kind of scale of reduction we should be expecting in other parts of our broader ‘suicide prevention system’ and should therefore be expecting in overall suicide numbers.

We then have “Within the last 10 years, we observed one of the lowest ever rates of registered suicides”. That’s true. And it cannot be emphasised enough that it’s a case of ‘observing’ this phenomenon. It doesn’t mean that having a (published) National Suicide Prevention Strategy since 2012 has driven this, as the ‘relatively low’ flat line has been observed since 2007.
Next it says “But we cannot ignore the fact that there is much more we can do”.
We absolutely cannot ignore that fact, and must not ignore it. And it’s not just a case of ‘doing more’, we need to ‘do different’ as well because what we’ve been doing since 2012, indeed since 2007, hasn’t been ‘working’ in terms of getting the suicide numbers on a downward trend.
The next sentence is very disturbing, and another massive fail when assessed against our Push change dynamic. It says “In 2018, there was an increase in the suicide rate following several years of steady decline”.
Referring to our chart again shows that the suicide rate did indeed go up in 2018 but not after ‘several years of steady decline’. And the overall picture is of ‘no reduction since 2007…after 25 years of steady decline’.
The final sentence in that opening section, after the Forewords, states “And while, overall, the current suicide rate is not significantly higher than in 2012, the rate is not falling. We must do all we can to prevent more suicides, save many more lives, and ultimately reduce suicide rates”.
This wording gives us a little more hope, as it emphasises that there is more we can do to reduce the number of suicides, including saying “we must do all we can” so there’s a bit of heart in there too.
But it’s half-hearted. There’s an emphasis on ‘suicide rates not significantly higher than 2012’ rather than ‘no reduction since 2012’; ‘preventing more suicides’ not ‘preventing all preventable suicides’; and ‘reducing suicide rates’ rather than significantly or considerably reducing the numbers.
Imagine the difference in Push power if it read as follows: “The overall suicide rate has not fallen at all since 2012. We must do all we can to prevent all preventable suicides, save thousands of lives, and get suicide rates on a downward trend (towards zero)”. Much more motivating!
NSPS Executive Summary — More Questions than Answers!
Next it’s the Executive summary, leading once again with that ‘considerable progress since 2012’ narrative; also including the line “We have seen one of the lowest ever suicide rates (in 2017)”, despite the trend not being down, so a selective use of statistics; and repeating the half hearted “However, while overall the current suicide rate is not significantly higher than in 2012, the rate is not falling. There is much more we must all do to save more lives”.
There’s a strong flavour in the document, and in the media interviews, of an emphasis on ‘personal responsibility’, eg the ‘suicide is everyone’s business’ message going out at the same time as government is not stepping up — indeed, potentially allocating fewer resources to suicide prevention in this NSPS 2023–2028)— with the ‘we must all do’ narrative then appearing to be a case of smoke and mirrors!
Add to this a classic of modern day politics, ie the tendency to quote lots of big £ numbers and give a scattergun list of activities, in both the document and in the media interviews when responding to scrutiny questions, and it makes the heart sink further.
It’s great that “All areas of the country now have local suicide prevention plans and suicide bereavement services” but not good that many local plans lack ambition — lots suffer from the ‘10% reduction in 5 years’ syndrome — and they lack the resources to deliver even a 10% reduction in the numbers.
And note that, once again, the feature item in this Executive summary is the 35% reduction in in-patient suicides.
As already commented, it’s definitely progress between 2010 and 2020, with some of this progress possibly driven by the National Strategy introduced in 2012, and it’s the kind of scale of reduction we should be seeking across the entire ‘suicide prevention system’ not just ‘the NHS system’ where the main focus of suicide prevention plans and activities has been historically.

In the final part of that first section of the Executive summary shown above, there’s reference to needing “a national government effort” as well as everyone else continuing to play their part.
Absolutely right, and the NSPS 2023–2028 suggests a weak effort from national government on this occasion.
It then goes on “The aim of this cross-government strategy is to bring everybody together around common priorities and set out actions that can be taken to…reduce the suicide rate over the next 5 years — with initial reductions observed within half this time or sooner”.
Firstly, is it really a ‘cross-government strategy’?
From what I’ve heard from those directly involved in putting this NSPS together, and from my own direct experience with several government departments, some are more committed than others, including some who display very little appetite for suicide prevention and tend to throw the ball back to DHSC rather than grabbing it and running with it.
And, as The Jordan Legacy has highlighted in its response to the NSPS 2023–2028, and in our report ‘Moving Towards a Zero Suicide Society’, and in our Suicide Prevention Act petition package for measures to minimise suicides, a true cross-government strategy needs to come out of a cross-government National Suicide Prevention Office (NSPO) — with teeth — not out of one government department, especially not DHSC, given the historic problem of suicide prevention being seen as ‘a (mental) health issue’.
And there’s The Priority Trap once again in that text “to bring everybody together around common priorities”. Far from helping us in getting the suicide numbers on a downward trend (towards zero), this could harm.
Yes, bring people together, link people together, join the dots, share experiences, share what works, innovate together, learn from differences in local circumstances, have better co-ordinated & integrated approaches, find ways to work in collaborative partnership in a new form of system, which we’ve framed ‘Everyone is a priority for someone’…but not just coming together ‘around common priorities’. That could cause harm!
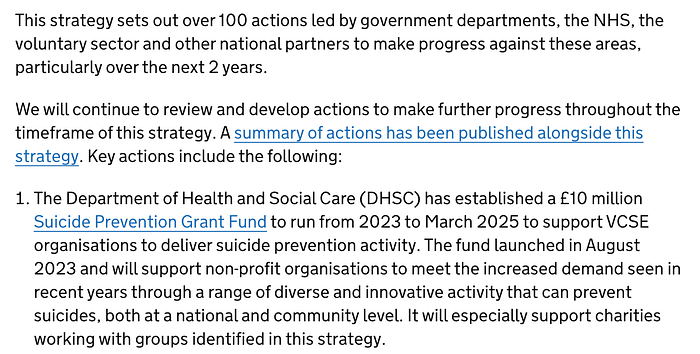
The Executive summary continues below with further featuring of the £10 million DHSC VCSE Suicide Prevention Grant Fund. Such funds are welcome, especially if they can be used for innovative ways of getting the suicide numbers on a downward trend, towards zero, and The Jordan Legacy put in a submission for this very purpose — to demonstrate our Zero Suicide Society Transformation approach — but DHSC said ‘no’!
Is this pot to fund innovation and breakthrough, or just more of the same?
It says here “The Fund launched in August 2023 and will support non-profit organisations to meet the increased demand seen in recent years through a range of diverse and innovative activity that can prevent suicides, both at a national and community level”.
So it does have the word ‘innovative’ in there. However, having read all of the detailed information as we completed the application, the emphasis is on funding operational activity (not capital investment) for existing services (not new services), so funding what is already being delivered.
There’s certainly opportunity to allocate resources to services, activities, projects or initiatives that are trying to innovate or ‘do something different’ to get the suicide numbers down and which can build the capacity of the system to be better at reducing the numbers, down towards zero.
But it looks like it might be primarily assisting with some prop-up funding for many existing services. And a one-off grant “to meet the increased demand seen in recent years” is problematic of course. Is it assuming that this ‘increased demand’ is a temporary blip and will fall away, so continuing funding will not be needed? That would be a dangerous assumption!
Also think carefully about that amount — £10 million.
In the bigger picture of suicide prevention — and the mental health crisis we’re facing — it’s a drop in the ocean.
The economic cost of each suicide death in England — taking into account police costs, coroners’ costs, bereavement counselling, the loss of an economically productive individual, the ongoing adverse impacts on those close to the person who’s died, etc — is estimated at £1.67 million.
https://publications.parliament.uk/pa/cm201617/cmselect/cmhealth/300/30005.htm
We should evaluate all these government announcements and programmes — and there are far more announcements than programmes! — against this economic cost as well as the clear human cost, including the fact that for every suicide death, an average of 135 people are adversely impacted, according to both Cerel’s research in the US and the Suicide Bereavement UK study (based on a sample of more than 7,000).
So that’s 5,000+ x 135 = 675,000+ people newly impacted each year, and compounded year-on-year.
The 5,275 suicide deaths registered in England in 2022 have caused immediate and enduring pain and suffering for 712,125 people, and cost the economy £8.8 billion — and, across the UK, it’s more than £10 billion.
So let’s keep £10 million for a Suicide Prevention Grant Fund in perspective! And also the £57 million being invested in the NHS Long Term Plan.
It’s good but it’s clearly not enough, and not enough in two ways. It’s not enough to get the suicide numbers on a downward trend (towards zero). And it’s not enough given the £8–10 billion cost pa from 5–6,000+ preventable deaths each year, which highlights there’s a strong ‘business case’ for much greater investment in suicide prevention.
Part of our Push change dynamic, part of our open expression of dissatisfaction with the status quo, must be highlighting this business case, this financial case, as well as the human and moral case, and saying this is simply not good enough…not accepting ‘we have limited resources’.
NSPS Ambition and Vision — or Lack of Ambition and Lack of Vision!
The next section of the document sets out the ‘ambitions’ and ‘vision’ for the NSPS 2023–2028— or does it?
Without a target for reducing the number of suicides in the next 5 years, and without signs of high ambition, and without the language of desperately wanting to get the suicide numbers down from the unacceptably high level they’ve been at for the past 15 years, it’s questionable if ‘ambition’ is the right word to use here. But let’s be literally accurate and say it sets out the low ambitions of the NSPS.
Does it set out a ‘vision’? Not in the sense of a clear picture of what our ‘finishing line’ looks like in 5 (or more) years’ time? Certainly not in terms of a compelling vision which can create the Pull change dynamic we need. It’s more a set of principles by which we could travel over the next 5 years.
And does this Strategy set out “the steps we will collectively need to take to achieve them (ambitions and vision)?” Not really, but maybe the more detailed action plans flowing from the Strategy will achieve that?
The principles set out (below) are largely ok. For example: suicide prevention does need to be a collective effort; and mental health should be as important as physical health; early intervention is vital; and “nobody should be left out of suicide prevention efforts”.
But the DNA of these National Strategies means they are fundamentally competitions for priorities with ‘winners and losers’ so many people do actually ‘lose out’!

Lived Experience Involvement — and the Democracy of Suicide Prevention
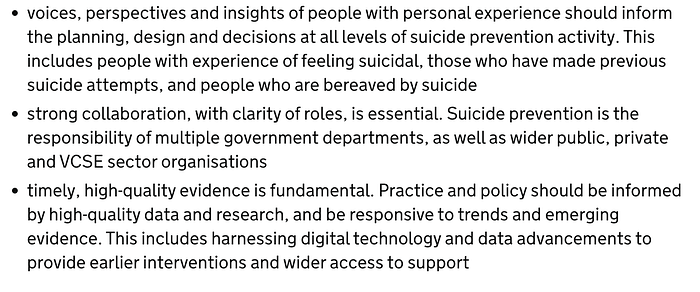
The “voices, perspectives and insights of people with personal experience” (see below) should most definitely “inform the planning, design and decisions at all levels of suicide prevention activity”.
This is the foundation stone for The Jordan Legacy’s Zero Suicide Society Transformation Model, and it should be front and centre for any national strategies and plans.
There’ve been improvements in this regard since 2012, although that’s not hard when there were just a handful of people with lived experience having input into that first published National Strategy in 2012 (some of those involved back then said “there were basically 3 people with lived experience advising, and their testimony was very powerful, but it was just 3 people”)…
…and the NSPS 2023–2028 definitely had more ‘Lived Experience Involvement’ than ever before…but still way below the wide and deep involvement we need.
We must guard against ‘satisficing’ or complacency. We mustn’t have low ambition in terms of Lived Experience Involvement, just as we mustn’t have low ambition in the Strategy as a whole.
Inevitably, some of ‘the privileged few’ who did have direct input into the NSPS 2023–2028 have praised the Strategy and praised the level of Lived Experience Involvement in its development, and praised the ‘ambitions’ for future Lived Experience Involvement.
This illustrates once again the crucial importance of wide and deep engagement to get the benefit of Involvement = Commitment, and why we must strive much harder and higher on Lived Experience Involvement.
We want many more people appropriately and effectively involved in shaping, and then implementing, strategies and plans, so more people feel involved, feel part of the process; so more people and organisations are committed to delivering on the aims, ambitions, goals and actions.
The very positive comments from some of those who were involved in the latest NSPS about the degree of Lived Experience Involvement suggest a degree of ‘capture’ as the privileged few involved this time have (subconsciously?) set low expectations and/or lowered their expectations.
As I highlighted earlier, Steve Phillip and I at The Jordan Legacy were formally invited to just a single online forum to have some input into the NSPS, on targets and measurement, and even on this one topic where we were asked for input, I’d say we weren’t really listened to. We were listened to by Jacqui Morrissey who hosted this NSPA forum but, ultimately, not listened to by the National SP Advisory Group, based on its decisions.
In our own networks — The Jordan Legacy’s networks, plus the personal networks of Steve and myself, and via those we closely collaborate with — we have around 600 people with lived or living experiences of suicide and, when we asked who’d been directly involved in shaping this new NSPS 2023–2028, there were 4. That’s 4 out of 600. That’s fewer than 1%!
Clearly, the NSPS process is still just scratching the surface on this key success factor for getting the suicide numbers down.
And let me make it crystal clear, I believe that we’re all just scratching the surface on Lived Experience Involvement.
I believe that myself and Steve and The Jordan Legacy are just scratching the surface because there are millions of people in our society with lived or living experiences of suicide, and thousands who are active in some way, so we must involve much wider and deeper than we are now.
We must avoid having the unhealthy situation where a small number of ‘lived experience voices’ — that includes us! — are being heard loudly and often whilst ‘the silent majority’ are not heard at all.
If we have a platform, we should try to use it to give others a platform.
If we are one of ‘the privileged few’ selected to have ‘a seat at the table’, we have a responsibility to find ways to involve others, not just bask in the glow of having a seat at the table or just focus on expressing our views.
We must avoid some ‘narratives’ being heard again and again, especially where these are neat ‘media friendly’ stories that fuel the soundbite culture and structure of our media, and yet other ‘stories’ not being told at all, especially where they are messy, multi-faceted, complicated, complex, including ‘mental health issues’ or suicide crises that had little or nothing to do with ‘mental health issues’ in many cases.
Just as in any other walk of life, we need to see this as a democracy and avoid any one person or small group of people having too much power and influence — whether that’s a small minority involved in an Advisory Group or a group or person directly advising government, or just being prominent in the media and on the speaking circuit.
It’s not healthy for the suicide prevention field to be such a hierarchy.
Quite rightly, people with lived or living experiences of suicide will be asked to ‘tell their story’ and they should grab every opportunity to do so, and do exactly that — tell ‘their’ story. Everyone has a unique ‘story’, and a unique ‘journey’, and no-one can have someone else’s experience.
We can only draw from our own experience, and we should be conscious of how our own experience shapes what we do and what we say, as well as — at a higher level of consciousness — what we’re not saying.
Of course, when we’re giving a talk or at a meeting with DHSC or sitting on an Advisory Group or appearing on the ‘red sofa’, we can talk about the ‘stories’ we’ve heard from others, we can summarise patterns and trends (as well as differences), we can draw from research and engagement exercises, we can share some collective experiences…but we’re still essentially talking from our own experience or, to put it another way, we are ‘experts in our own experience’.
In a democracy, we must always take care about representation, including self-representation, representing others, and being represented by others.
In what is often disturbingly called ‘the suicide prevention sector’ — becoming a distinct, organised ‘sector’ has some advantages but brings with it plenty of problems too!— we often hear claims of ‘representing others’ or ‘being a representative’ for others, with meetings often beginning “I’m here representing…” followed by a particular demographic group or socio-economic category or community of interest or geographical area.
On many occasions, this person has no democratic legitimacy at all, no right to speak on behalf of others. In reality, they’re speaking for themselves, and we should all be honest about this, starting with being honest with ourselves, as well as being entirely comfortable about this.
We need to provide more opportunities for more people with more diverse experiences to tell their ‘own story’, and shape suicide prevention strategies and plans, and delivery programmes, plus reviews and evaluation.
A few people will have the democratic legitimacy to speak on behalf of others, eg a democratically elected representative, or Chair/CEO of a member organisation with transparently accountable processes, or a universally recognised community leader with a track record of listening widely and deeply to their community members before speaking on their behalf, or a formal nominated proxy, eg a carer speaking on behalf of the person they care for.
But, talking of ‘care’, we must all take care on this point of ‘representation’, and spend more time giving a platform to others rather than using our platform and claiming to represent others.
It’s been very healthy to have recent meetings with the National Suicide Prevention Alliance (NSPA) and to both acknowledge that we need to go much wider and deeper than currently to have appropriate and effective Lived Experience Involvement. That even where we mark our report card as ‘good’ or ‘better than in the past’ or ‘better than for any previous National Strategy’, this has to be followed by “but can and must do much better”.
And, hopefully, those who’ve enthused about this new National Strategy’s ‘commitment to Lived Experience Involvement’ will be coming from the perspective that we need to raise the bar much higher, not have ‘more of the same’ or more low expectation satisficing because we’ve had a bit of involvement for a (still) privileged few and had our tummies tickled!
Because of my passion for and vast experience in ‘the democracy field’ over the past 40 years, I’ve offered to work with NSPA and others in producing a “deliberative and participative democracy map for the suicide prevention landscape” — which can also include ‘representation democracy’ and ‘direct democracy’ where relevant — and drafting a strategy for how we can widen and deepen Lived Experience Involvement with the highest of aspirations.
Now back to the detail of the National Strategy document…
Collaboration not Competition, Innovation not Inertia!
The NSPS rightly highlights the importance of collaboration and there’s massive scope to improve collaboration as well as removing the barriers to collaboration and tackling destructive competition in the field of suicide prevention. Ironically, some organisations that regularly call for greater collaboration are very selective in who they collaborate with!
That final bullet point above also needs carefully unpicking.
Many might just read it and agree — yes, high quality evidence is important, as is being responsive to trends and emerging evidence, as is harnessing digital technology and data advancements for more effective, earlier interventions and better support.
But there are a few issues here.
Sometimes there’s too much focus on having lots of ‘evidence’, and new ideas are stifled.
To ‘do something different’ — and we must do some things different to get the trend line from a flat line to a down line! — we need to back new ideas, especially where people with lived experience are telling us what might help prevent suicides, and then start to build new evidence bases.
The traditional response from the academics and policymakers who’ve dominated suicide prevention strategy in the past has been to knock back any ideas that don’t yet have a ‘strong evidence base’ and to stifle new ideas by saying, often disingenuously, “what are the ethics of doing this?”.
Effective suicide prevention needs a culture that embraces new ideas; and, if the idea is one that sounds like it might save lives, we should all be asking “what are the ethics of NOT doing this?”.
Advances in ‘Tech for Good’ and ‘Digital Life Saving’ have suffered in particular, held back by traditionalists saying ‘where’s the evidence base?’ and ‘what are the ethics of doing this?’ and also by fuelling narratives like ‘technology isn’t the answer, people need human connection’, ‘people who are suffering don’t just want an app’ and ‘AI isn’t the answer to everything’!
These narratives are unhelpful, at times destructive, and they’re stopping us from saving lives.
These narratives are often fuelled by people who are not that familiar with the latest developments in ‘Digital Life Saving’, or digital communications technology generally, and who perhaps even feel threatened by it.
Those actually working in the ‘Tech for Good’ and ‘Digital Life Saving’ fields appreciate more than anyone that we need integrated digital-human solutions, eg with the technology identifying someone who needs human support — at crisis and/or early intervention stage — and directing those who need help to the sources, including human support, that they need.
Those developing ‘Tech for Good’ services around the known needs of people generally and particular sub-groups or segments of the in-need population know that ‘it isn’t just about an app’.
The background of these ‘app developers’ is increasingly in ‘user experience design’ and developing customer-focused services so when they apply their skills and experience, often driven by a personal suicide loss or personal mental health crisis, they’re totally focused on developing a very human, person-centred tool with digital-human integration and synergy, with the technology being very much a means to the ends, not an end in itself, although valuable human-centred technology developments which are groundbreaking technologically is clearly a motivator too.
When a leading adviser to government and ‘the suicide prevention sector’ recently ended his annual summing up with the line “AI isn’t the answer to everything”, I cringed because it’s such a silly thing to say as well as continuing to fuel these unhelpful, potentially harmful, narratives.
Of course ‘AI isn’t THE answer to everything’ just as ‘technology isn’t THE answer to everything’ but it is AN answer, it’s one of the tools we have in our suicide prevention toolkit, and we should be embracing this opportunity to develop new tools and new applications of established tools by utilising this new Tech for Good.
Once we engage with those working in Digital Life Saving & Tech For Good, we find, for example, there’s a useful distinction between AI as Artificial Intelligence and AI as Augmented Intelligence, with many augmented intelligence data solutions being brilliant extensions of what the suicide prevention traditionalists do as well as completely new in some cases, eg studying patterns in financial data to identify people at risk of suicide, or in danger right now, so we can get them instant, targeted support.
In my meetings with the Digital Life Saving & Tech For Good communities, I find a much more balanced perspective between tackling the (potential) harms of the online world and developing the (potential) helps of the online world.
And one of the ‘private sector’ developers we’re currently working with has developed systems to protect ‘whistleblowers’ — or ‘ethical champions’ as I prefer to call them. The ‘public sector’ often treats the ‘private sector’ with suspicion, in what is just prejudice or a sweeping generalisation, and sees itself as the guardian of ethics and protector against ‘online harm’. In this case, a ‘private sector’ solution is helping those experiencing harm in the private sector and those experiencing harm in the public sector!
Also, when the suicide prevention traditionalists talk about the online world, it’s usually heavily weighted to talking about ‘online harms’ and advocating for ‘more research into the impacts of online harms’ and ‘measures to tackle online harms’. In this negative culture, it can be hard to get the positive ‘help’ perspective on the agenda.
It reminds me of Martin Seligman, the author of the bestselling books Learned Optimism and Authentic Happiness, having his big light bulb moment when someone sitting next to him on a plane said “so you’ve spent 30 years studying what makes people unhappy and depressed, do you ever study what makes people happy?”. The Positive Psychology movement was born!
Aims, Objectives, Goals…Action!
The final part of the Introduction section of the National Strategy document concludes with ‘Aims’.
Once again, this includes the “overall ambitions” which don’t look at all ambitious, and with no quantifiable targets for reductions in suicides.
The National Strategy may feel positive and hopeful to the small number involved in drafting it, because they may have more faith in the people and institutions behind it but, for the rest of us, the whole document seems to require a ‘leap of faith’ — at a time when we have little faith in government.
And aims like “continue to improve support for…” are so non-specific and non-committal, they provide little or no insight or confidence.
The document also occasionally includes positively-worded text such as “Suicides are not inevitable and collectively we should, and will, aim to prevent every suicide we can” and “…it is imperative that government departments and other organisations responsible for delivering suicide prevention activity are accountable for the delivery of these actions…”…
…but the rest of the document doesn’t give any convincing indication that these are anything more than words in a PR-oriented document.
The “summary of actions, setting out the basis for an implementation plan” reads like a long wish list without the resources to deliver.
Also, the prevailing philosophy from all those involved is ‘limited resources, so must set priorities’ rather than ‘must do all we can to get these numbers down (towards zero)’.
The final paragraph above, and comments we’ve heard from people who are involved with the Advisory Group, is that ‘in many respects, the process is really just starting now, in getting into action plans and delivery plans’.
So there we were on 11 September 2023 thinking ‘we finally have a new National Strategy after a 12 months’ delay’ but we’re hearing at the end of November/beginning of December that “we’re really just starting now”!
Of course, some action plans are continuations of previous plans and don’t necessarily need major work or recasting but, as there’s been no reduction in suicide numbers for 15 years and we need to ‘do something different’, it sounds like there might still be a lot of preparation needed to even get to the new start line for the approach that will deliver reductions at scale.
The Priority Trap plus Other Biases and Barriers to Suicide Prevention
As I comment from here, there’s a danger of people thinking ‘he’s just repeating himself now’ although, in my defence, the document does itself have some of the same points in ‘the main body’ and in the Executive summary and, in a few cases, in the Forewords too…
…and, just as the authors of the National Strategy probably felt these points needed repeating and emphasising, I feel that my criticism of some of these points also needs repeating and emphasising!
If you feel you’ve seen enough evidence of the National Strategy’s low ambition, unhelpful language and framing, and potential for harm as well as help, and all the flaws in the National Strategy process, you might want to skip to the final section, and my call-to-action at the end.
If you want to know more of the finer details and ‘hidden traps’ in the National Strategy/National Strategy process — potentially sub-conscious ‘hidden traps’ for even some of those involved in shaping it and drafting it! — please read on.
I’ve already highlighted ‘The Priority Trap’ with the entire National Strategy process being like a huge competition for priorities, with ‘winners and losers’, with privileged ‘winners’ and desperately sad that there are so many ‘losers’ when we’re talking about suicide prevention here, literally life or death decisions being made.
As we say in our Zero Suicide Society Transformation Model, and in The Jordan Legacy’s response to the NSPS for England, 2023–2028, we need a collaborative, co-ordinated approach to suicide prevention around the principle of ‘Everyone must be a priority for someone’.
Those of us committed to a truly compassionate as well as ambitious transformation programme to get the suicide numbers on a downward trend, towards zero, know that we simply cannot have ‘losers’.
The Government, and those conspiring with them, can choose to have ‘winners & losers’ but that just emphasises that the Government is just one piece in the puzzle and its National Strategy is just one piece in the puzzle.
And this then emphasises why we must not simply roll over and say “let’s just implement the National Strategy” or “let’s just align our priorities to the National Strategy’s priorities”.
This would mean that as well as getting into bed with low ambition, failing your ‘local constituency’ and endorsing the approach of ‘pushing air around in the balloon while the overall numbers of suicides don’t come down’, you’d be conspiring in a process of systemic discrimination, which I’ll say more on below.
Many people will probably read the first paragraph in the section on ‘Priority areas for action’ (below) and think it sounds reasonable.
After all, setting priorities and determining actions based on ‘evidence’ and ‘data’ is what most people — in government and elsewhere — do as generally accepted good practice for generations, along with “engagement with people with expertise” in the subject and then, a more recent development in the field of suicide prevention, engaging with and involving “people with personal experience”, what we usually now refer to as ‘lived experience’ along with what are often referred to as ‘other key stakeholders’.

However, what this means in practice is that there are a series of systemic biases designed in, consciously or subconsciously.
First, there’s the bias towards whatever ‘evidence’ or ‘data’ exists, and a bias against any issue or group or potential solution where there’s currently little or no ‘data’ or ‘evidence’.
This happens frequently. Where there’s an established data set showing a high suicide rate among Group X, attention focuses on Group X. Where it’s suspected that Group Y has a high suicide rate, but there’s no hard data on this yet, attention continues to focus on Group X, not Group Y. As long as the data gap remains, the discrimination against Group Y continues.
Second, a view is taken, consciously or subconsciously, on what determines ‘expertise’ in suicide prevention, ie who is an ‘expert’ and what exactly we mean by an ‘expert’ in suicide prevention?
Historically, it’s tended to be a small group of academics, clinicians and policymakers who’ve largely come from within the health system. With many, if not most, of the academics also having a background largely in the health system, the systemic bias to health is well-embedded, including the ‘Department of Health’ overseeing suicide prevention strategy, despite us knowing suicide is not just a (mental) health issue.
The bias can be even worse where the academics, clinicians and policymakers involved not only share largely a health background, but more narrowly a mental health background and sometimes even more narrowly a professional psychiatric background.
And, traditionally, the academics involved in these national strategies and plans have a background in analysis of quantitative data. Their ‘expertise’ has been built up on years and years of analysing large data sets of historic suicide statistics and analysing large population sets to identify ‘patterns in the data’ and identify ‘risk groups’ and recommend policy solutions.
Of course, we have all sorts of other ‘experts’ in non-health fields, in other forms of data analysis, in predictive modelling, including the latest AI based models, in real-time response to real-time data, in qualitative research, in behavioural research, in transformational change, etc.
There are many other types of ’experts’ who could help us determine how we can get the suicide numbers on a downward trend, towards zero, drawing from their diverse disciplines, including getting the benefit of ‘fresh eyes’ on a problem that clearly needs different approaches because the approaches we’ve been taking for the past 15 years haven’t been getting the numbers of suicides down.
The third source of potential bias and discrimination, of course, is the selection of “people with personal experience, researchers, and those involved in the planning and delivery of services”, including who gets to be a member of the National Suicide Prevention Strategy Advisory Group (NSPSAG).
As I’ve said in my talks and webinars many times, the ‘system’ operating here is based on the fundamental principle of there being ‘a table’ and a select group of people ‘getting a seat at the table’ with a competition, overt and covert, to gain power by getting ‘a seat at the table’…
…but the table is never going to be big enough to have diverse perspectives; many of those at the table are ‘representing’ a particular viewpoint, constituency or issue so are effectively like a ‘lobby group’; there are many people and organisations without a ‘seat at the table’…
…and maybe the solution is not to have ‘a table’ to stop people trying to fight for one of the limited number of seats there?!
Through my analysis and commentary around the NSPS below, I’ll cover — with specific examples from the NSPS document— the many other systemic biases and discriminatory practices that have been designed-in to this process, whether deliberate or a case of unwitting design flaws or unintended consequences; and the many pitfalls in the NSPS process.
First, let’s study some content of significance in this section:
Wider Community Engagement and Public Consultation
There’s a reference here to “The responses to our engagement exercises, such as the mental health call for evidence, roundtable discussions, and many ongoing discussions with experts…”.
There’s such a low degree of transparency and accountability in this process that the overwhelming majority of those who work in suicide prevention and/or have lived experience and take an interest, never mind the population as a whole, have no idea who these ‘experts’ are who’s shaping policy, apart from the very visible few like Professor Appleby, or who’s involved in these “roundtable discussions” or who sits on the Advisory Group — a question regularly asked in online forums and on social media but I’ve never seen it answered, and it should be published somewhere — or who’s been engaged by whom.
As I mentioned earlier, of around 600 people with lived experience of suicide in our networks, we found 4 who had been directly engaged in the National Strategy process; and the only invite Steve Phillip and I had to be directly involved was the one-off NSPA online forum on “targets and measurement” which was then largely ignored I’d say.
And then there’s the issue of public engagement or public consultation dedicated to suicide prevention. There was nothing at all in England, in stark contrast to the excellent model rolled out in Scotland.
Those responsible for the National Strategy for England have tried to defend their position by saying, and continuing to say, ‘but we had the Mental Health Plan consultation and we got lots of comments through it about suicide prevention’; and the National Strategy document refers to “…our engagement exercises, such as the mental health call for evidence…”.
This is probably the best example of the huge gap in thinking and expectations in what is good practice in public engagement around suicide prevention; around the adequacy of what was put in place in England; and around an appropriate culture & structure for ‘engagement & involvement’.
The public consultation on the 10-year Mental Health Plan was a public consultation by the ‘Health Department’ about mental health.
There was no dedicated, cross-departmental, public consultation focused on suicide prevention which, as we all know is not just a mental health issue — and such engagement should be co-ordinated by someone other than the ‘Health Department’ to avoid that systemic bias.
The public consultation around the Mental Health Plan was structured around 6 questions the public were asked to respond to. None of these 6 questions was explicitly about suicide or suicide prevention.
The final question was focused on crisis services and support, so implicitly suggested that we might be talking about suicide and suicide prevention, but still didn’t explicitly mention suicide or suicide prevention here.
And nowhere else in the briefing around these 6 key questions, these 6 key chapters in the discussion document, was it explicitly asking for views on suicide prevention, just a passing reference to the Mental Health Plan consultation also being an opportunity to input into the Suicide Prevention Strategy with, at that time, no timetable set out for the new National Suicide Prevention Strategy and no indication of how views expressed might influence the Suicide Prevention Strategy.
Note how in the discussion paper briefing (above), it also indicates who DHSC were wanting to hear from. Once again, no explicit mention of suicide or suicide prevention.
It was like reading a corporate wellbeing strategy for a multinational corporation that dances around the subject of suicide with lots of references to wellbeing, mental health, mental health conditions…extending as far as referring to mental ill-health…but no explicit mention of suicide or suicide prevention, for fear of frightening the horses!
Not great leadership by example is it?!
Of course, many people used this only available opportunity to input their experiences and ideas around suicide prevention.
Those in the ‘inner circle’ like Professor Appleby, Tweeted that this was an opportunity to shape the new Suicide Prevention Strategy, but the fact that it wasn’t structured explicitly around suicide prevention — it wasn’t structured appropriately to get relevant, high quality input directly into a Suicide Prevention Strategy — meant it was not an effective engagement process, just a way of generating ad hoc comments. Useful comments in many cases but ad hoc and not a good practice engagement process.
In Scotland, there was a two-stage process with both stages dedicated to the Suicide Prevention Strategy specifically, which from the outset had been a collaborative initiative between the Scottish Government, the Convention of Scottish Local Authorities (COSLA), a multi-agency steering group, and a lived experience advisory group.
Stage One was a ‘blank sheet of paper’ exercise to hear evidence, experience, and ideas for what should be in the Suicide Prevention Strategy. Stage Two was a consultation around a draft Strategy which was published for comment. Nothing like this in England.
And then, in England, we had the announcement there would not now be a 10 Year Mental Health Plan but, instead, mental health was being merged into a broader Major Conditions Strategy, with the previous engagement responses for the Mental Health Plan ‘being taken into consideration in the shaping of the Major Conditions Strategy’ with a new “call for evidence to inform the Major Conditions Strategy” issued on 17 May 2023.
So expecting people who’d previously commented on the Mental Health Plan, thinking there was going to be a separate Mental Health Plan, to now comment on a new Major Conditions Strategy, and anyone wanting to focus specifically on suicide prevention effectively seeing their topic of focus being swamped by other huge issues like cancer and dementia.
And still nothing explicitly on suicide prevention at this stage, with nothing emerging until the National Suicide Prevention Strategy for England was published on 11 September.
The document that was released on 11 September could easily have been published as a ‘draft Strategy’ inviting comments and suggestions. Then everyone would have had the opportunity to input, shape the National Strategy, and feel more a sense of ‘ownership’ of it perhaps.
I suspect that the Government — for which we might read DHSC and its Advisory Group — didn’t do this for the following reasons.
Firstly, it might not even have thought of it because it doesn’t have stakeholder engagement and lived experience involvement at its core. For some, this would be uppermost in their mind.
Secondly, it might have thought about it, and thought ‘we don’t have the resources to do this’ but that’s actually the Government saying ‘we’re not going to give suicide prevention a priority’ and allocating the necessary resources to do the right thing.
Thirdly, the ‘scarcity mindset’ of those involved in this National Strategy process, operating within a mental model that’s focused on setting priorities, is likely to have made them think ‘if we open this up to public consultation, we’ll get everyone arguing their case for being a priority and it’ll be a high profile bun fight’. Indeed, I’ve actually heard at least one civil servant say this out loud.
Let’s again deconstruct this language, this thinking, and let’s think of alternative perspectives and narratives.
What the public consultation process around a draft Strategy could have given us is greater transparency, more accountability, a more democratic process, a more inclusive process — with opportunities for the Government, DHSC, the Advisory Group, to hear more and more diverse perspectives, gather more evidence, hear the case for different approaches or a different focus, hear about ‘emerging evidence’, listen to new ideas, etc.
And, to repeat, in our Zero Suicide Society model, within the co-ordinated, collaborative ‘everyone must be a priority for someone’ approach, we’re not just seeking to allocate scarce resources to ‘priority groups’.
So, in our mental model, we’re entirely comfortable with an open public consultation around a draft National Suicide Prevention Strategy, inviting challenge. The only reason ‘the establishment’ isn’t comfortable with such an approach is because it’s boxed itself in with its own thinking.
Priority Areas for Action — and the Dangers of the Prioritisation Model
Now, back to the document, back to ‘their world’, and ‘priorities for action’.
It’s easy to read each of the 8 points below and agree and say these are all important and these might all get the suicide numbers down but there are many flaws that we should at least be conscious of; and it’s very hard to argue these are the most important 8 that we should give priority attention to and allocate ‘scarce resources to’.
Why these 8 and not another 8?
And note the ‘get out clause’ in inclusion of the word ‘include’.
This ‘priority’ list is not an inclusive list, which brings into question why call it a priority list? Of course, if they lengthened it to make it more inclusive, so it got to 15 points or 20 items or 25 actions…well it ceases to be a list of ‘priorities’ doesn’t it?
It’s more evidence of being stuck in the ‘priority mindset’.
As this dissertation I’m writing is a critique of the National Strategy, let’s go through each of these with a ‘critical thinking’ head on.
Prioritising data and evidence can lead to reductions in the suicide numbers but it can also potentially lead to a bias against the kinds of new ideas that can provide breakthroughs in suicide prevention.
Focusing on ‘priority groups’ can mean neglecting other groups, effectively discriminating against other groups, possibly even harming other groups.
Just as we’ve identified harm in categorising patients in hospitals as ‘high risk’ and ‘low risk’ — with those categorised as ‘high risk’ getting the support they need and those categorised as ‘low risk’ then being more likely to end their lives because we’ve categorised them as ‘low risk’ !— having ‘high risk’ groups, and therefore ‘low risk’ groups, in a National Strategy is potentially harmful for those who are categorised as ‘low risk’.
“Addressing common risk factors linked to suicide at a population level to provide early intervention and tailored support” looks good on first reading but mainly because this is the accepted wisdom that has guided policy for 50 years. However, in terms of reducing suicide numbers, this approach stopped working 15 years ago — see our ‘flat line chart’. The world has moved on but policymakers haven’t moved on with it.
It’s the same mindset that applied to commercial marketing for 50 years and gave us the great TV advertising campaigns in the 1970s and 1980s. It’s the same mindset that was applied in many fields, from market research to epidemiology. But, in the digital age, commercial marketers don’t just look at the population level, identify groups or market segments, and then devise strategies and campaigns for these groups or segments, they target individuals who are more likely to buy the product or use the service.
In suicide prevention, we can identify a ‘population group’ or ‘target audience’ and devise strategies or group-based communications — and, in some cases, this might work, although it hasn’t ‘worked’ for 15 years in terms of bringing the national suicide numbers down — but, to save lives, to get the suicide numbers down, towards zero, we need to more effectively communicate with ‘individuals in danger’ not just ‘groups at risk’.
Of course, we can shape a broad policy response for a broad group, but it needs more targeting, including to the individual level.
We know that a very high ‘risk group’ is middle-aged men but people don’t end their life because they’re a middle-aged man. We know that middle-aged men are more likely to have certain ‘high risk experiences’ such as divorce or redundancy, so we can devise strategies and campaigns that focus on helping people who are experiencing divorce or redundancy, and we should have this kind of ‘behavioural’ or ‘experiential’ targeting, as the most effective commercial marketers do.
But then we still need to focus on the individual middle-aged man who’s experiencing divorce or redundancy right now. Our strategies and systems should be set up to make sure we’re communicating with this ‘active target group’ and the individuals within this group.
Our success in saving lives and getting the numbers of suicides down, towards zero, will be partly a result of our ability to have the right strategies, policies, plans and generic practices for all middle-aged men having these experiences — as well as any more upstream prevention that’s possible, eg avoiding destructive redundancies — but it will also very much depend on our ability to identify, communicate with, and support individuals in danger because they’re experiencing divorce or redundancy, or whatever the primary experience is, in ‘real time’.
“Tailored support” can be structured at a group level, but must be delivered at an individual level — something I learned from working in, for example, the funerals industry in Australia where you can have ‘preactive’ plans and packages for a range of types of funeral, ready to activate when there’s a death and ‘you get the call’, but then each funeral, within each ‘package’ must be completely tailored to the individual ‘customer’.
On the 4th point around online safety, I’d agree that ‘tech for bad’ and reducing online harm is something we need to tackle but we also need to invest much much more in the field of ‘Tech for Good’ and ‘Digital Life Saving’ to harness the latest technology in order to save lives.
The ‘suicide prevention sector’ is generally not good at embracing technological development, sometimes resistant to it, and with quite a few prominent Luddites who are quick to destroy even the possibility of technological enhancements with their (conscious or sub-conscious) unhelpful, even harmful, comments like “technology isn’t the answer” and “people need human support not an app or machine learning”.
I’m the first to agree that “technology isn’t THE answer” but it’s AN answer.
I also agree that ‘people need human support’. These apps and machine learning and augmented intelligence solutions to suicide prevention are often designed to more quickly and effectively identify people who are a suicide risk or in suicide danger, then get them the appropriate human support they need as quickly and effectively as possible.
It’s not a war between humans and machines. It’s not a war between public services & charities focused on compassionate human support and private companies focused on their technical gizmos and making money.
These are destructive, prejudiced, outdated stereotypes. We need an outbreak of peace; and a spirit of collaboration among all those — and there are many — with a shared sense of mission around getting the suicide numbers on a downward trend, towards zero.
Yes, of course, we need to provide more and better crisis support, and we need to do much more to avoid people getting to crisis point.
Yes, of course, we need to reduce access to the means of suicide, and to reduce access to lethal means, and — again — be much better at upstream suicide prevention to minimise the number of people getting as far as a suicide attempt and therefore needing us to restrict access to means.
In our Zero Suicide Society model, restricting access to means is within a broader category of ‘Designing Out Suicide’ or ‘designing in suicide prevention’. There’s so much more we can do here, including a full scale review of planning guidelines and the Building Regulations from a ‘suicide safer’ perspective. Past reviews of the Building Regs have focused on ‘safety’ from the perspective of trying to prevent accidents. We should take another look from the perspective of trying to prevent deliberate self-harm.
“Providing effective bereavement support to those affected by suicide” is another ‘no brainer’. We know how traumatic it can be to lose someone to suicide and there should be ‘wrap around care and support’ for those affected. And we’re getting better with this, but with much more scope to improve.
We also need to think more about those experiencing bereavement in all its forms, including all forms of traumatic loss, because it’s not just bereavement by suicide that has adverse impacts which lead to a heightened risk of suicide, eg men aged 85+ losing their wife who they’ve been married to for 50+ years.
Whether their wife has died by suicide, from cancer, or a heart attack or stroke, these men are a high suicide risk and should have the full ‘wrap around care and support’ package.
And, finally from the list of 8 ‘Priority Areas for Action’ is “Making suicide everybody’s business”. Again, I totally agree that everyone can help in suicide prevention and we need more people providing help, although — as outlined earlier — we need to be careful to use the right, most inclusive language, ie avoid the preachy, finger-wagging ‘suicide is everyone’s responsibility’ and the more-likely-to-get-pushback ‘suicide is everybody’s business’ and use more engaging language like:
anyone can be affected by suicide, everyone can help prevent suicides
This next paragraph is another example of the ‘good but could be much better…and could go much further’ nature of this low ambition Strategy.
‘Encouraging everyone to review their plans and approaches’ is not a set of words to provide confidence that appropriate and effective action will be taken. Neither is ‘continuing to promote cross-sector working and joint action’. It would be easy for anyone in our target audience here to ignore.
And why should “everyone — including employers, local government, NHS and VCSE organisations…ensure alignment with this new strategy”?!
All employers, councils, NHS Trusts, VCSE organisations, etc who are committed to minimising the number of suicides among their employees or the people they care for or the area they cover should be looking at what they need to do in their workplace, area, hospital, etc to minimise the number of suicides and look at this National Strategy to see if it could help them to achieve their goals, or have no benefit, or even potentially harm their suicide prevention efforts, eg if their ‘priority groups’ are not listed as ‘priority groups’ in the National Strategy…
…and then decide whether to align with the National Strategy or ignore it or publicly speak out against it where it’s preventing suicide prevention, as I’m doing here of course.
Improving Data & Evidence — and the Data & Evidence Bias
Clearly having better data to guide suicide prevention strategies, plans and actions is an ongoing challenge and so ‘always a priority’ for improvement.
We do need to think more though about the biases and discrimination within the National Strategy process and ‘establishment suicide prevention activity’ due to the focus, at times obsessive focus, on ‘data and evidence’.
I’d say the most important sentence in this next section is the final sentence “Future work must continue to address evidence gaps to inform more effective actions” because the National Strategy is a bit like a patchwork quilt that’s full of holes.

To reiterate two points highlighted previously…
Some ‘priority groups’ are well organised, or ‘the system’ is well-organised on their behalf, and we have access to high quality, insightful data, or are being presented with high quality, insightful data and evidence; and these groups are being given priority — for action, for further research, for inclusion in policy development, for funding, etc — effectively discriminating against other groups where we don’t (yet) have the data and evidence or where these groups are not (yet) organised enough, or not (yet) effective enough in lobbying, to be considered a ‘priority for action’.
There’s a bias against anything new, against new ideas for reducing suicide, against new groups coming forward, against new technological development…because being new, by definition, there often isn’t (yet) any ‘data or evidence’.
Sometimes there is, eg when it’s a new suggested approach based on existing data and evidence but, even then, ‘the new’ is looked upon sceptically, especially by those who’ve been involved in these National Strategy processes for many years, because they’re often ‘blind spots’.
Sometimes it really is completely new, different, innovative, even breakthrough thinking where there really is no data or evidence yet. The response — and I’ve experienced this personally many times — is usually to “go away and gather the data and evidence to support it”.
A more helpful response would be “how can we help you gather the data and evidence”! After all, every established, evidence-based, data-supported approach had to start somewhere as a new idea or hypothesis to test.
The ‘suicide prevention establishment’ — and I use the term ‘establishment’ deliberately because of its culture & structure — is quick to knock back new ideas, especially where they involve technological change, or anything they don’t fully understand or don’t feel they can control, with lines like “Ah, but is this evidence-based?” and “Ah, but what about the ethics of doing this?”.
We need a complete change of mindset, where new ideas for suicide prevention are welcomed and embraced, especially where they come from people with lived or living experiences of suicide, ie from the ground-up — always the biggest threat to any establishment! — and where any new suggestions, in good faith, for preventing suicides and reducing the number of suicides is responded to with this line instead:
this idea/suggested approach/new use of technology for suicide prevention could save many lives, so what are the ethics of NOT doing it; why would we not enthusiastically embrace this proposal and run with it?
The next section — screenshot below — continues with the systemic bias and discrimination of the National Strategy process, with “particular groups” highlighted as being ‘priority groups’ for improving data and evidence.
They’re all important of course but for every group highlighted and prioritised, there are others not highlighted and not prioritised and therefore discriminated against.
Here’s just two examples of ‘groups’ of people with heightened suicide risk who rarely, if ever, feature in these national strategies and plans.
Firstly, older people, eg men aged 75+ who take their own lives for various reasons, including losing their lifelong partner and declining physical health. There are plenty of gaps in the data and evidence for this group, but they tend not to feature.
Secondly, people losing their jobs. At least men aged 75+ in theory have organisations like Age UK who could gather data and evidence and advocate on their behalf — although I haven’t seen much evidence of this — but not ‘people losing their jobs’.
There isn’t an organisation for people losing their jobs. There isn’t an organised lobby group to put their case to the powers-that-be or to the suicide prevention establishment.
They aren’t really ‘a group’ at all, just individuals dotted around the country, across all ages and socio-cultural groups, who happen to have two things in common: they’ve lost their job and they’re at heightened risk of suicide.
These people are overlooked and discriminated against in the National Strategy process, and within our political system more widely.
They sometimes feature in local suicide prevention strategies because some parts of the country have high unemployment rates and local analysis of suicides has shown unemployment to be a significant factor.
And this is why much suicide prevention activity must be ‘from the ground up’ — and why some local suicide prevention partnerships or local organisations might not want to ‘align’ too closely with a National Strategy that doesn’t reflect local issues and drivers, and may even not include a local ‘priority group’ at all.
Real Time Suspected Suicide Surveillance (RTSSS)
Thankfully, we finally have Real Time Suspected Suicide Surveillance (RTSSS) and local partnerships coming together around this data and the actions that need to flow from a better understanding of what’s driving suicides and what can be done to reduce, to minimise, the numbers.
Many of us have campaigned for this for 10 years or more, and it’s been sad to watch ‘the suicide prevention establishment’ resisting it until the arrival of COVID19 and, more particularly, the Lockdowns, caused a shift of thinking and practice that’s now made this a reality.
There are a few theories about why RTSSS was resisted for so long.
Some say ‘we needed to get it right, get the right systems in place, get the data right’, etc — which is a common problem in suicide prevention, as in other fields. At worst, it’s the search for near perfection before acting, rather than acting and seeing how it works, or piloting to test how it might work, including using dynamic formative evaluation designed to help make it work rather than passive, detached, summative evaluation designed to check whether it works. And did this process really need to take 10 years?!
There are those who say that some people or organisations within the suicide prevention establishment resisted RTSSS because it meant they would no longer have ‘control of the data’. I’ll let you reflect and decide on that one.
Meanwhile, I’m grateful we now have it, nationally and locally, and it’s potentially a breakthrough in suicide prevention, but please use it for ground-up analysis and tailored action in your area, don’t fall into the trap of continuing to be driven by what national data is telling us:
And let’s also avoid other traps that allow low ambition to breed. Having RTSSS data should empower us and energise us to aim higher, and get those suicide numbers on a downward trend, towards zero.
One danger from ‘establishment thinking’ is believing that our role is now to monitor this new real-time data to see where numbers might be rising and take remedial action to stop them rising and bring them back to our familiar flat line, rather than constantly aspiring to reducing the numbers, towards zero, and using the data to help us achieve that goal.

What the national RTSSS data has given us is an extension of our flat line graph so we know that it’s no longer 15 years of no reduction in the annual suicide numbers, it’s 16 years of no reduction in the suicide numbers.
This is unacceptable, and we must all be dissatisfied with this status quo, certainly not ‘celebrating’ the numbers not being higher or getting excited at new data for its own sake.
All data and evidence is simply a means to an end — in this case, the end of getting the suicide numbers on a downward trend, towards zero — not an end in itself although, as a Research Fellow, I know that researchers often see having high quality, insightful data as an end in itself, sometimes forgetting it’s actually just an input into a process, a means to our ends.
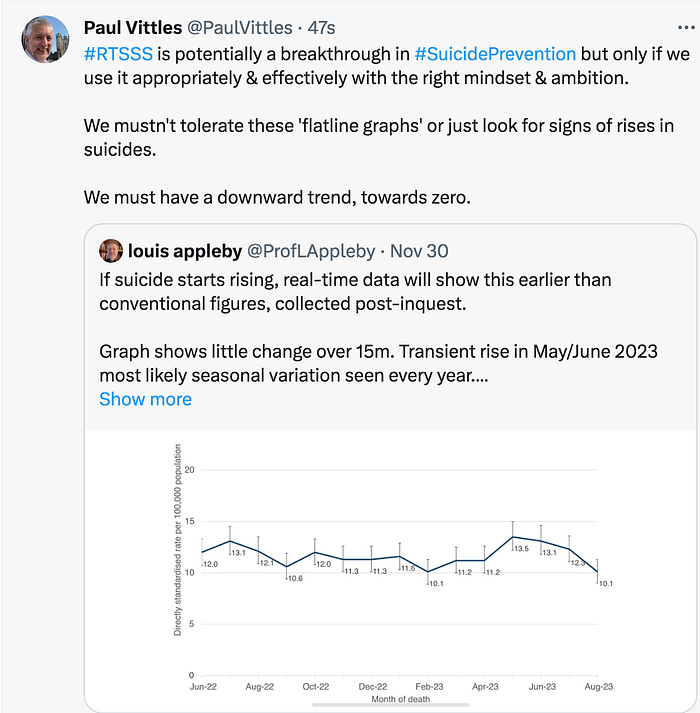
More Data & Evidence Bias — and Selection Bias
Obviously, a key role of Government is to conduct and commission necessary research to provide exploratory or explanatory data that enhances our ability to reduce the number of suicides, towards zero.
Again though, there’s a problem with the systemic biases and discrimination that takes place when certain groups are prioritised.
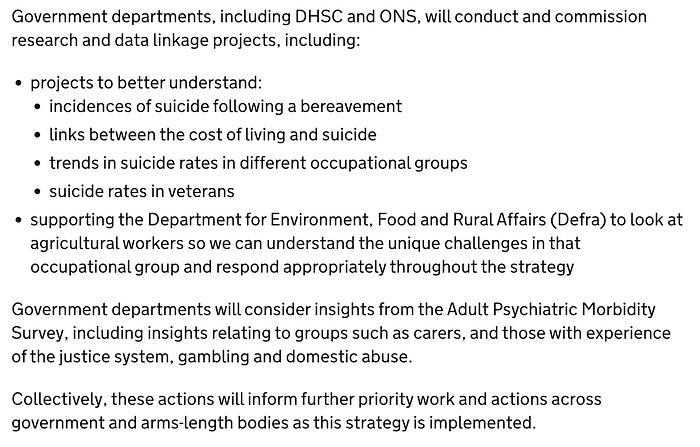
We need to better understand incidences of suicide following a bereavement but this can be interpreted by those working in suicide prevention quite narrowly, usually studying where there is or might be heightened suicide risk among people bereaved by suicide, but not studying heightened risk among those bereaved by conditions or circumstances other than suicide, eg (older) people losing a lifelong partner to cancer or dementia.
Also, historically, the health bias in suicide prevention research has discriminated against research into socio-economic factors.
In the past few years, there’s been a bit more attention given to socio-economic factors, including broad relationships between the unemployment rate and the suicide rate in recessions or the relationship between suicide and poverty, but much of this research is simply number-crunching using existing datasets showing correlations, with perhaps some attempt to identify causation, but always highly qualified with caution.
What’s usually missing is the qualitative research and deep insights that shed light on these inter-relationships, the chain of causation, and what can be done to prevent suicides among those living in poverty, or those struggling to pay bills, or those who’ve just lost their job.
What’s also often missing is ceteris paribus research where we study a sample of people who’ve had a similar experience in apparently similar conditions but with a different outcome, eg a sample of people who’ve lost their jobs and been unemployed for 3–9 months where some have taken their own life and some haven’t, to understand what might have caused those who ended their lives to do so, and others not.
In very recent times, it’s “the cost of living” which has become the primary narrative and it’s an example of another systemic bias in the National Strategy process. It tends to pick up ‘topical issues’ at the point where a new National Strategy is being discussed and developed, like ‘the cost of living’ and ‘online sources of harmful drugs’ and pull them in to the published National Strategy; with other issues, which may or may not be just as important, not getting on to the agenda. This reflects the way that Government works generally of course, not just suicide prevention.
Another key bias of the National Strategy process is this concept of ‘having a seat at the table’ for ‘the privileged few’ who get to influence National Strategies and plans. In the past month, it was announced — once again through the only source we seem to have for information about the National Strategy, Professor Appleby’s X/Twitter account — that the charity Money & Mental Health now has ‘a seat at the table’:

These charities ‘getting a seat at the table’ are all fine charities and I want them all to be having input but, again, we must be conscious that, within the current system, these are 3 ‘winners’ and there are many more ‘losers’!
Btw, I’ve noticed at least a dozen posts and questions asked at relevant events asking “who’s on the Advisory Group?” (ie the National Suicide Prevention Strategy Advisory Group) and I’ve never seen the question answered. Is there a reason for this apparent lack of transparency and accountability? Is there a list published somewhere?
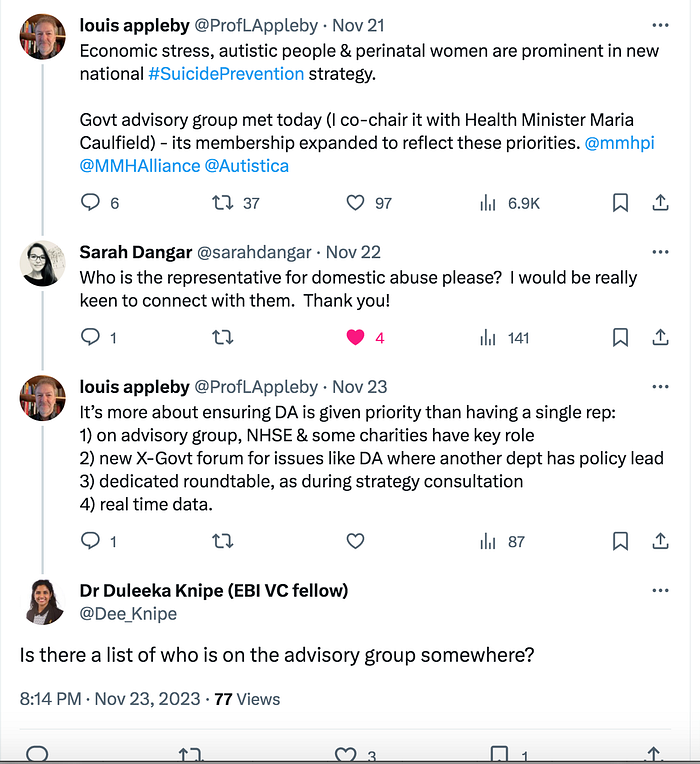
The Information and Accountability Deficit!
There’s certainly a gaping hole in terms of accountability as no-one seems to have responsibility for communicating to the world outside the inner circle what the Advisory Group is discussing and recommending.
On the issue of ‘targets and measurement’ for example, NSPA published a summary of the online discussion that it facilitated on this particular topic but the Advisory Group didn’t publish a response or explain why, after receiving this input, it chose not to have a reduction target.
I’ve raised this with a couple of people who I know are members of the Advisory Group, and they don’t seem to think it’s an issue, so emphasising that they view the world through a different lens to the many people not members of the Advisory Group who, in contrast, think that an information flow with summaries of what’s being discussed and agreed by the National Suicide Prevention Strategy Advisory Group is a minimum expectation.
And saying, as they did, “we don’t have resources for that” is a weak response!
Quantitative Analysis, Qualitative Insights, and Research-Backed Action!
Back to the National Strategy document!
It says Govt/DHSC/ONS “will conduct or commission research or data linkage projects, including…trends in suicide rates in different occupational groups”.
Now, I’d be the first to say that, to get the suicide numbers down, towards zero, we need to look at different occupational groups, and this is also part of our Zero Suicide Society model.
But one of the biggest frustrations with Government research is that it’s often number-crunching without actionable insights or highlighting specific actions that can be taken to reduce suicides or it’s monitoring of trends which clarifies what the problem is without necessarily providing solutions. At worst, ‘trend analysis’ simply tells us that there’s been a slight increase here and a slight decrease there whilst the overall numbers of suicides is the same…and we haven’t progressed at all.
Government should be working in collaborative partnership with different sectors and professions with the clear aim to reduce the numbers, including any further research needed. In many cases, no further research is needed, it’s action that’s needed, so ‘trend analysis’ can be naval gazing. In other cases, specific targeted action research would be useful.
The Construction sector is an obvious one to partner with, given that almost 10% of all suicides are people working in Construction, although I can’t see it explicitly referenced in NSPS 2023–2028. Add in those working with the Construction sector, it’s probably 1 in 7 suicides.
Now here’s another problem. I’ve attended meetings with some of the suicide prevention establishment in the past and when you say something like “probably 1 in 7 suicides”, their response is “we’re not sure if that number is correct and we need to do more research to check if it is in fact 1 in 7”.
An alternative response would be “yes, it’s probably around 1 in 7, and we know for sure that 500 people working in Construction die by suicide each year, and we know that people working in Construction are 10 times more likely to die by suicide than by physical accidents at work; we don’t need any more data to tell us there’s a problem here; how can we get these numbers of suicide deaths down significantly, and on a downward trend (towards zero)”.
Then we have “suicide rates in veterans”. This is another example of where it’s possible more or different research is needed, but we also have a lot of research, and a lot of knowledge from lived experience, pointing to actions we can take to reduce the number of suicides, so we often just need more action not more research.
The ‘scarcity mindset’ often causes further problems here, where people are, from the outset, looking for evidence of what to prioritise and how to prioritise, ie ways of limiting action, rather than being action-oriented.
And, last but not least, we have “agricultural workers”. Do we really need more (quantitative) research among this group? Why? To find out what? What actions can we take now to reduce suicides among agricultural workers that doesn’t need more data or more quantitative analysis?
Gaps in the Data and Data Quality
In the penultimate paragraph, we’re informed that “Government departments will consider insights from the Adult Psychiatric Morbidity Survey” (APMS). I understand this will be a new APMS, published in 2024, to provide up-to-date data and new insights.
That might be useful, especially if there’s wider engagement with key stakeholder groups, including people with lived experience, to make sure we’re asking the right questions to the right sample, although ‘the experts’ will probably want to keep these ‘technical matters’ to themselves.
It’s hard though when surveys like the APMS take place so infrequently, with the last one being in 2014, with some government departments, and charities like Mind on their website, still quoting some statistics from the 2007 APMS as if they’re the latest figures.
The world has completely changed since 2014, including being turned upside down by the COVID19 pandemic. It’s quite bizarre to still be developing plans, policies, campaigns, etc based on 2014 data.
No self-respecting commercial organisation would be basing decisions on data that’s almost 10 years out-of-date. HM Treasury wouldn’t be basing economic policy on data from 2014. Why should we be relying on data to underpin decisions on suicide prevention strategy from a 2014 survey?
Because of the lack of up-to-date data, The Jordan Legacy has been working in partnership with MEL Research to carry out a twice a year survey among a representative sample of 1500 UK adults to give us up-to-date data, and trends, on key figures around suicide and suicide prevention.
But we shouldn’t have to do this. There shouldn’t be a gap to fill.
If the Government was truly committed to suicide prevention, it would make sure key data was collected annually — or, at the very least, every 2–3 years — and trends monitored.
Again, it’s good that we’ll have the new APMS data in 2024 but not good that a National Suicide Prevention Strategy has been developed in 2023 in the absence of this data.
While we’re on the subject of the APMS, I’d just like to highlight a pattern I’ve observed throughout my research career. These types of Government surveys are often highly sophisticated in their sample design and analysis to help provide high quality, reliable, representative data, but they often have poorly designed questions so undo the good work on sampling.
In my workshops, I often talk about the art and science of survey research. The sampling component is largely science with a bit of art. The question wording component is more of an art mixed with science.
As the screenshot from the APMS report below shows, the questions are rather strange and with potential biases.
“Have you ever thought of taking your own life?” would be a reasonable question on its own but what is probably a large ‘design committee’ has added “even though you would not actually do it?” which then just makes the question confusing.
After getting a ‘yes’ response to “have you ever thought of taking your own life?”, we can ask something like “did you seriously want to end your life?” or “did you make a plan to end your life?” or lots of other clearer questions that would give us a more accurate and less ambiguous set of answers.
Similarly, it’s a perfectly good question to just ask “Have you ever made an attempt to take your life?” so why then add “by taking an overdose of tablets or in some other way?”?
I can imagine the ‘survey design committee’ arguing that this addition clarifies what’s meant by a suicide attempt and/or tries to get the widest possible definition, but is it really necessary and does it bias responses, eg those taking overdoses more likely to answer ‘yes’?
Surely just the first part of the question needed?!
I digress…
Tailored & Targeted Support — or Institutionalising Priority Group Bias
Back to the National Strategy document again; back to ‘priority groups’; back to the problem of bias and discrimination due to the fundamental driver of the entire National Strategy being setting priorities.
As I’ve highlighted elsewhere, the systemic bias is deeply embedded in this whole process, eg where certain groups are selected for ‘priority status’ whilst other groups, like older people, are excluded completely, and then the Strategy demands that for the selected priority groups “It is therefore crucial that organisations and individuals tailor and target resources and services to support these groups”.

In other words, it’s urging other people and organisations around the country to embed this constructed bias and discrimination, rather than focusing on the groups in their area or community of interest who they regard as needing particular attention…or simply treating every group at risk and every individual in danger as worthy of support.
While we’re on the subject of ‘The Priority Trap’, the inherent biases in the National Strategy process which can be counter-productive and potentially harmful, and the ‘top-down’ mentality that often drives these National Strategy processes, despite us now having some excellent local suicide prevention partnerships looking at ‘real time data’ in their areas and being able to react to local circumstances and be more effectively ‘preactive’, ie better prepared to react where being proactive is difficult…
…it’s worth just highlighting that the Government’s lead adviser on suicide prevention strategies, plans and policies, Professor Appleby, is very much from the ‘old school’ tradition of top-down, population data-driven, priority-setting, strategic planning.
In this presentation to the BMA, Prof Appleby tells the audience what he thinks the priorities should be, including priority groups to focus on, for the next 10 years; and he describes his thinking, his process, and his advice, which of course is the kind of advice he’s giving to government.
Just have a think about this.
In the fast-moving, ever-changing world we live and work in, with much uncertainty, and events like the COVID19 pandemic hitting us — only now in the Inquiry are we getting proper insights into the decisions taken, or not taken, and why — and technological transformations taking place whilst only just scratching the surface of AI, and with opportunities to build from the ground up with RTSSS-centred local partnerships and micro zero suicide plans…are we really in a position to say which groups should be a priority for the next 10 years?
And should we? How would this help? How might this harm?
Professor Appleby will often inform audiences in his presentations — and he delivers many presentations, including always being a keynote speaker, some would say the keynote speaker, at NSPA Conferences — that suicide is complex with many different causal and contributory factors, which is absolutely the case, but then he’ll also argue for focusing the National Strategy on a few ‘priority groups’ and a few ‘key drivers’.
The problem with these types of process is that as soon as you prioritise specific groups or particular actions or ‘key drivers’, you discriminate and introduce a bias that can harm as well as help.
In the National Strategy document, in addition to explicit prioritisation, there are several instances where it gives examples, or says ‘especially’ or ‘particularly’. On each of these occasions, a bias is created or reinforced.
It may be helpful, it may be harmful, helpful to some, harmful to others.
We need to be conscious that the bias is there and be sure we feel justified in creating or sustaining such a bias as well as thinking about alternative models with a co-ordinated approach where ‘everyone is a priority for someone’ and there’s a more flexible ground-up system.
Of all Professor Appleby’s Tweets, this one is perhaps the most disturbing:
Not only does the Government’s lead adviser on suicide prevention believe that we should set out priorities for the next 10 years, and build a National Suicide Prevention Strategy around ‘priority groups’, but he believes that the list of priority groups “has to be short to be meaningful”.
And this is at the very heart of the problem with this traditional mindset in government, in our institutions generally, and in the process used to devise our National Suicide Prevention Strategies…where you have a ‘scarcity mindset’ and believe that every process is about identifying priorities and allocating scarce resources.
You want to agree on as small a number of priorities as possible to have, and to demonstrate, impact, so you can continue to argue for further priority-setting, ie ‘we prioritised young people and we’ve reduced the suicide rate among young people’.
But not only does this process discriminate, it’s been proven over the past 15 years to not bring down the overall number of suicides— it just pushes the air around in the balloon — and, worse still, it doesn’t even have a good track record of reducing suicides in some of the ‘priority groups’, eg young people were given priority status in the previous National Strategy but rates have been rising among young people.
And, sadly, this can lead to a ‘doubling down’ effect where lack of progress encourages those caught in The Priority Trap to argue for a smaller number of priority groups to try and have more impact within these groups, ie fewer winners and more losers!
Here’s the list of ‘winners’ in the latest competition for priorities that we call the National Strategy process. As you look at the list, please study the ‘winners’ and also think about who the ‘losers’ are this time.

As I’ve highlighted a few times now, the list includes children & young people and middle-aged men, but not older people or older men, despite men aged 75+ having a substantially higher suicide rate than men aged under 25. Again, I’m not advocating for any one group to be given a higher priority, just highlighting the bias, and advocating for a co-ordinated approach where ‘everyone is a priority for someone’.
It’s easy to make a case for each group to have some degree of focus, but also easy to argue a more inclusive case. For example, we know that many new mothers struggle but then so do new fathers. We know that there are people in contact with mental health services who need better support but also people not in contact with mental health services who are desperate to keep out of psychiatric services because of the harm they can cause, eg having a young anorexic girl placed in a general psychiatric ward.
It’s good to see more attention being given to autistic people, with emerging evidence that it could be 1 in 10 people taking their own lives, or more, who are autistic. But what about people with other neurodivergent conditions? Why specifically autistic people and not, say, people with ADHD? Again, to what extent does this narrow prioritisation help or harm?
Not Trying to Cover Everything in the National Strategy from Here!
Just a quick note here to say that, for the remainder of this critique of the National Strategy, I’m not going to try and comment on every part of it, just those parts I feel warrant comment, and content that illustrates the broad criticisms I’m making, eg around ‘The Priority Trap’; ‘The Top Down Trap’; the bias and discrimination embedded in the process, and what’s not included; the systemic low ambition; barriers to suicide prevention that are created or sustained by the National Strategy and its process; and the failure to have positive change dynamics built in to the National Strategy.
I don’t comment specifically on the sections in the National Strategy on people who’ve self-harmed; alcohol & drugs misuse; people with chronic physical illness or physical health conditions; the broader issues around children & young people, other than schools and higher education; crisis support; or the ‘responsible portrayal of suicide in the media’.
I’m not neglecting any of these issues or groups, or giving them lower priority in any way. They’re all important ‘pieces in the puzzle’, and they should all have a section in the National Strategy.
The main reason why I’m not commenting specifically on these issues/groups is that I largely agree with the content in the National Strategy document, and I welcome it.
Risk/Causal/Contributory Factors
Another key bias historically has been the health bias in the lens through which suicide & suicide prevention are viewed and the structural approach to suicide prevention, which is seen as the responsibility of the Health Department, the NHS, and the health profession.
Anyone new to suicide prevention soon sees that suicide is not just a (mental) health issue and there are many causal and contributory factors.
It doesn’t take long for anyone with their eyes open, and their mind open, to see that factors like those listed below, and factors like poverty, are drivers of suicides.
Those steeped in the world of suicide prevention talk about ‘socio-economic risk factors’ or ‘socio-economic determinants’ of suicide.
Most citizens will recognise these factors — in plain language — as not having enough money to feed the kids or pay the bills and getting little or no support from government, being (made) homeless, being made redundant, feeling completely alone, etc.
It’s not rocket science, but it is science and it’s art too, as just a bit of creative compassion quickly identifies people who are struggling and the situations and environments in which they’re struggling.
The more we focus on ‘cure’ rather than on prevention, the more we focus on crisis and ‘crisis interventions’, the more we focus on downstream problems rather than on upstream solutions…the more we end up looking through that health lens again and not making much progress.
At the heart of solutions for getting the suicide numbers down from the unacceptably high level of 6,000+ preventable deaths every year in the UK, 5,000+ preventable deaths in England each year, down towards zero, are these underlying factors or determinants. They are central not tangential.
As the National Strategy document states “Links have been evidenced between suicide and social determinants of health such as housing, poverty, employment and education” but, again, please carefully study the language used here.

The Health Bias, Socio-Economic Factors, and Suicide as a Political Issue
Firstly, “social determinants of health”.
These are socio-economic and socio-political determinants of suicide. Calling them ‘determinants of health’ is part of the continuing health bias, like slipping suicide prevention as an incidental item into the consultation around the Mental Health Strategy rather than having a dedicated suicide prevention engagement process.
Secondly, people seem to run away from the reality that suicide is political. Not party political — we don’t want a destructive party political bunfight — but suicide is political, eg people living in poverty are more likely to die by suicide, and poverty is a political issue, so suicide is a political issue.
Thirdly, personal & political beliefs have a massive bearing on suicide prevention strategies, plans, policies, practices…and communications around suicide prevention, including advocacy and campaigning.
Many people and organisations constantly focus on suicide as a personal responsibility, talking about people ‘needing to be more resilient’ or initiatives ‘to help build resilience’, and saying people should ‘reach out’
Other people and organisations (also) see suicide prevention as a collective responsibility and collective endeavour, with a significant role for government and our institutions, with a degree of individual resilience-building needing to be combined with fundamental improvements to the circumstances, conditions, and environment in which people live and work (or don’t work because they can’t get work) so individuals don’t have to keep summoning up huge reserves of personal resilience to just survive.
Constantly asking people to ‘reach out for support’ demonstrates a complete lack of understanding of what it’s like being in the depths of depression and suicidal despair. People don’t ‘reach out’ at this point. They can’t reach out at this point. That is the point! We must ‘reach in’ and get better at ‘reaching in’, not keep expecting these people to ‘reach out’!
Fourthly, think about this statement from the section of the National Strategy below: “We encourage everybody working in suicide prevention to consider the wider determinants in their efforts to prevent suicides”.
‘Consider’? They should be at the heart of suicide prevention strategies, plans, policies, and activities, not just be ‘considered’!
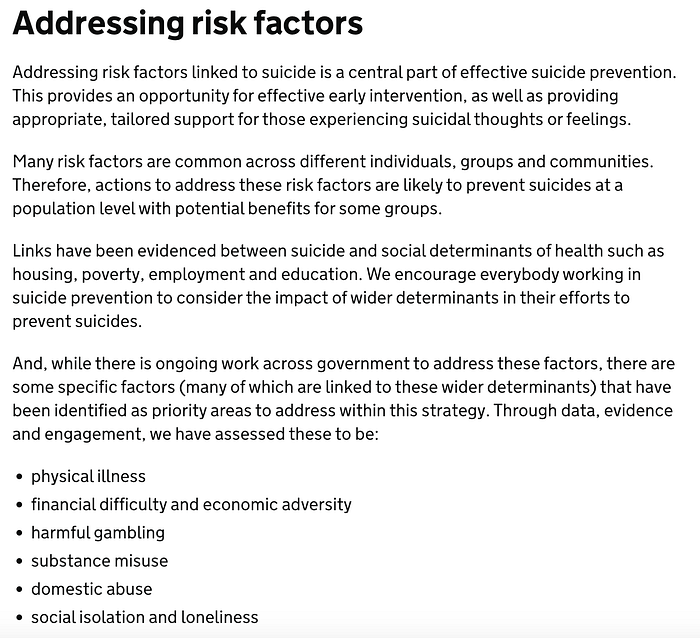
And, of course, prioritising the ‘risk factors’ has many of the same flaws, pitfalls, risks and potential harms as having ‘priority groups’, including the problem of ‘data and evidence bias’ I highlighted previously.
The text below is more hopeful as it’s through collaboration and local plans that much of our success in reducing the number of suicides will come, although important that local suicide prevention plans are ambitious — Zero Suicide Plans! — and focus on local issues, local drivers, local data and evidence, local ideas and suggestions, and local priorities where they feel the need to focus…not just aligning to ‘national priorities’.
It’s absolutely crucial that local collaboration brings “a wide range of partners together”, and experience suggests that local partnerships tend to be much more inclusive than involvement at the national level.
It’s also absolutely crucial that local partnerships take into account “wider determinants linked to suicide prevention, such as housing and financial difficulty” and, again, the evidence shows that local partnerships are much better at doing this than at the national level.
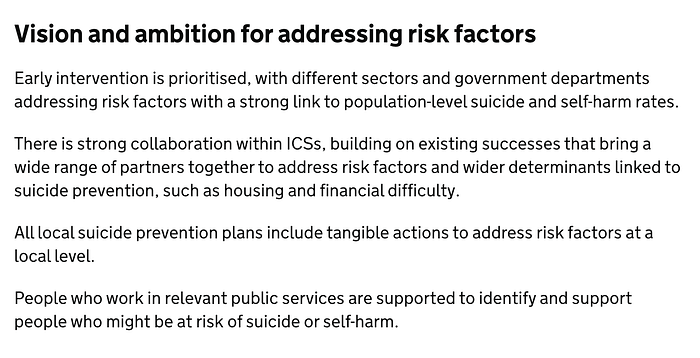
I’ve already commented on the DHSC VCSE Suicide Prevention Grant Fund, welcoming this opportunity — although putting this £10 million fund into perspective when preventable suicide deaths cost the UK economy more than £10 billion every year — and saying I’d like to see a focus on innovation and breakthrough ideas rather than just revenue funding existing services which, at worst, could just be propping up unsustainable services.
I also wanted to add here, or emphasise here once again, the inherent bias in this entire process, and the potentially harmful ‘winners and losers’ approach from the priority group-centred mentality.
The DHSC Grant Fund seeks applications from local VCSEs that focus on ‘the national priorities’. The OHID wants “local plans in line with national priorities”. The NHS Long Term Plan funding is designed to support “specific groups”. And so it goes on.
Local partnerships and local plans that are developed from the ground up based on local issues and then co-ordinated locally can generate a different picture to local plans feeling they have to align to national plans, national priorities, and especially, national funding.
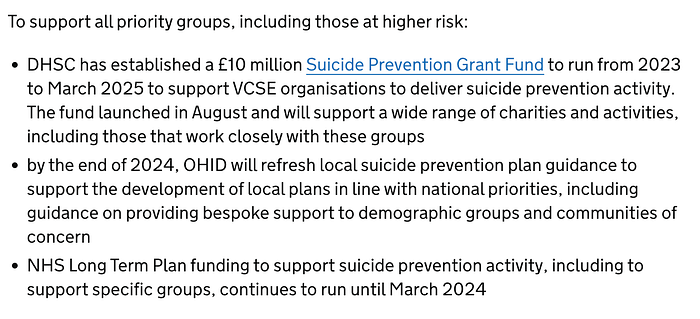
Suicide Education in Schools for Suicide Prevention
Virtually everyone we speak with in our suicide prevention work, and virtually everyone we interviewed as part of our action research project in 2023, believes that suicide education in schools is a key piece in the puzzle, and many say “it’s a no brainer”.
The 3 Dads Walking petition to have suicide prevention as part of the schools curriculum got 170,000 signatures — one of the highest numbers of signatures for any petition to parliament — and, in the parliamentary debate it prompted on 17 March 2023, there was almost universal support for this proposal…until, that is, the DfE provided a cool response and said it would consider “whether” to take this proposal forward.
Many months later, when the National Suicide Prevention Strategy was finally published on 11 September, DfE is still saying “whether” in the Exec Summary and, below, “reviewing RSHE guidance to consider the inclusion of suicide and self-harm prevention as an explicit part of the curriculum”.

It’s not very heartening or hopeful to still be talking ‘whether’ not how we implement this ‘no brainer’.
Young people, and often very young children, are already exposed to suicide & self-harm. They’re already talking about suicide & self-harm, and already engaging in self-harm behaviour, and 1 in 15 have made a suicide attempt by the age of 17, according to the UCL Millennium Cohort Study.
Not having suicide and self-harm as an explicit part of the curriculum would be irresponsible.
Suicide Prevention in Higher Education
Another petition launched via The LEARN Network by parents who’ve lost their children after they went to university, arguing for a statutory duty of care, had widespread support, getting 128,000 signatures, but it had strong pushback from the higher education sector and lukewarm support or even opposition from some of the bigger suicide prevention charities — some of whom work closely with the universities and either genuinely didn’t believe that a statutory duty of care would help save lives or didn’t want to rock-the-boat in terms of their relationships with universities, or both.

This month (December 2023), Maggie & Robert Abrahart will be in the High Court arguing their case for a statutory duty of care, as the University of Bristol appeals against the County Court decision that it effectively contributed to Natasha Abrahart’s suicide
It’s possible that the courts will rule against a statutory duty of care, and it’s possible that other measures will be taken by universities to create a suicide-safer environment and get the numbers of suicides down, but it’s also clear that the group of people most knowledgeable on this topic, ie the bereaved parents — intelligent people, some of whom have worked in the higher education sector — believe that it’s only through a statutory duty of care that we’ll get change, and get change quickly. Any delay in making this change is putting more students at risk.
Those from within the higher education sector arguing against a statutory duty of care, and those from the ‘suicide prevention establishment’ arguing against having a statutory duty of care for universities, often include in their argument against this proposal — and the Government’s lead adviser on suicide prevention has made this same comment publicly on several occasions — that the suicide rate among students at UK universities is significantly lower than for the population as a whole. And it features again here in the National Strategy document:
Whilst appearing to support action to prevent suicides among university students, it adds a preamble “While ONS statistics suggest that higher education students in England have lower suicide rates…”.
This is code for ‘so not a priority’. In the minds of those who think and operate around the need to limit actions to those that are ‘evidence-based priorities’, this is their staple diet and instinctive reaction whenever anyone suggests action to reduce the numbers of suicides among university students…to effectively say ‘it’s not really a problem to be solved’.
This is a very painful message for bereaved parents to hear, and bereaved siblings and others who’ve lost their family members or friends to suicide at university; and it’s needless pain and a needless comment; and it doesn’t help anyone apart from defensive higher education institutions that are not fully committed to preventing all preventable suicides.
If we approach this issue from a Zero Suicide Society perspective, ie trying to do all we can to prevent all preventable suicides and ‘move towards zero deaths’ in the higher education sector, then it doesn’t matter what the relative suicide rate is between university students and the general population (of people of a similar age). It’s irrelevant. It’s not helpful to even mention this. In fact it’s harmful to mention it. So why do it?!
We need mandatory Zero Suicide Plans for all higher education institutions so they all try to do all they can to prevent all preventable suicides. We need that level of ambition and commitment, and we need the National Suicide Prevention Strategy to include this level of ambition and commitment. We don’t need a National Strategy that sends a message to universities or anyone else that there’s not a problem to be solved here because suicide rates among university students are ‘relatively low’!
Considering Problematic Biases due to The Priority Trap
Let’s look at some of the other ‘priority groups’ in the context of “yes, of course, there needs to be action to reduce the numbers of suicides among people in these groups but just focusing on a small number of ‘priority groups’ is not going to get the suicide numbers down towards zero, and may be harmful”.
Firstly, middle-aged men.
Whenever I read text like this below re prioritising ‘middle-aged men’, my first three thoughts are:
- yes, we need to reduce the numbers of suicides among middle-aged men but people don’t die because they’re a middle-aged man, they die because of common experiences that middle-aged men are more likely to have and we must focus on these experiences with experiential and behavioural targeting;
- we also need to reduce the numbers of suicides among younger men and older men, because we have suicides here too, and every life is equally important — despite some politicians and commentators clearly believing that older people were ‘expendable’ during the pandemic! — and so we also need specific plans for younger men and older men, ideally Zero Suicide Plans tailored to their needs and circumstances;
- we also need to reduce the number of suicides among women — women of all ages — and, given that women are significantly more likely than men to attempt suicide, we must have ‘suicide attempt prevention’ strategies and plans for women of all ages as well as men.

Of course, the suicide prevention establishment doesn’t think like this — and doesn’t adopt a co-ordinated, collaborative approach where ‘everyone is a priority for someone’, as it believes ‘not everyone can be a priority’ in its winers and losers competition.
Two other thoughts I have when reflecting on the above text from the National Strategy, especially the line about middle-aged men having had the highest gender-age-specific suicide rate since 2010, ie for the entire period of the Government’s published National Strategies since 2012, which may sound like unfair criticisms, and I’m trying hard to avoid personal criticism of individuals who I’m sure will be acting in good faith:
1) if they’ve been a ‘priority group’ for attention since the very beginning, why have the numbers of suicides among middle-aged men not fallen?
2) from the content in the document, it still reads like they don’t understand the underlying issues and they don’t know what to do.
This is partly the health/health system bias causing this of course, because so many of the contributory factors and, especially, the underlying causes of suicide among middle-aged men are not health issues.
All the middle-aged men we lost in my own community in Teesside in the early 1980s — previously strong communities and big, strong men, systemically ‘de-hoped’ by the ideologically-based economic policies of the Government of the time — were not driven to suicide by ‘health issues’!
The paragraph below begins to get under-the-surface somewhat but it smacks of naivety and reflects what tends to happen in a system that is largely crisis-focused and health-focused.
It’s very common for ‘financial difficulty’ to be narrowly interpreted as ‘in debt’ and needing ‘debt counselling’ or ‘debt support’. Debt counselling is an important service, and there are some excellent debt counselling services available, and many people can be helped with “debt support”.
However, many of those in financial crisis are in a situation where they can’t meet their basic needs with the income they have and no amount of ‘better budgeting’ or ‘debt management’ can change this situation.
If we’re truly committed to doing all we can to prevent all preventable suicides, we’d be advocating for policies like a Universal Basic Income or Guaranteed Minimum Income, and appropriate reforms to the ‘benefits system’ (including not calling them ‘benefits’!) that will tackle the underlying problem rather than just trying to manage the symptoms.
As I’ve highlighted earlier, there are also fundamental problems with expecting people in distress and danger to “disclose that they are experiencing thoughts of suicide or self-harm”…to DWP!
The focus in this National Strategy on DWP being reactive not proactive is highly disturbing.
In the suicide prevention field, there’s often far too much emphasis on urging people to ‘reach out for help’ when we know that people who are in vulnerable situations, and certainly in suicidal crisis, don’t ‘reach out’ so need us to ‘reach in’.
So we need DWP and other public services to be proactive.
Of course, what we really need to ‘move towards zero suicides’ is a complete transformational shift in the entire culture and structure of institutions like DWP, away from a modus operandi of ‘give out as little money as possible, make it as hard as possible to get money, shame people for not having a job or independent financial means, and humiliate them on a regular basis to keep them from challenging the system’ — my characterisation for effect, but many people’s actual experience!
We should be shifting to a system where we do everything possible to support people in need; help them get (back) into suitable work as quickly as possible; listen carefully and empathically and with respect to people in need; proactively inform people about what support is available and help them to get it as painlessly as possible; help people to live independently with the highest possible quality of life, with opportunities to thrive beyond survive; do everything possible to ensure optimal (mental) health and prevent suicides because that’s the human thing to do and it saves the taxpayer lots of money in the long-run.
I read the study, referred to below, among middle-aged men — which was useful, and the specific actions outlined below will help — but two thoughts that kept going through my mind are, firstly, that this kind of research is so rare, despite middle-aged men having had a heightened suicide risk for decades and, secondly, the report highlighted the massive problem of stigma whilst fuelling a contrary message that ‘men are opening up’.
Many campaigners have used this report to ‘challenge the myth that men don’t talk and men don’t seek help’, arguing ‘this report shows that men are talking about their mental health and seeking support for their mental health’, and yet one of the key findings in the research was that men were opening up about their mental health issues and suicidal thinking after first making appointments to see their GP about a physical ailment. In other words, stigma and shame are still a huge problem, and the system discriminates against mental health issues.
I can draw from my own personal experience here in knowing that the entire system demands of people they diagnose themselves before even being considered for an appointment with a doctor and, even then, it’s often an initial telephone call or video call with a junior doctor — or “trainee” (self-described in my case) — and people are much more likely to get access to a GP (and I mean ‘a GP’ not ‘my GP’) by saying they have a tangible, specific, physical ailment rather than being honest about the emotional and psychological torture they’re currently wrestling with.
So we need fundamental ‘systems change’, we need transformational change, but we get a few transactional adjustments proposed alongside a misleading narrative about ‘men are getting better at seeking help and we should encourage more to seek help’.
Let’s unpack this: “Each of these interaction points provides additional opportunity to prevent suicides and encourage middle-aged men at risk of suicide to seek the right support”.
Yes, each interaction point is an opportunity, and not just for middle-aged men. We should be identifying and enhancing every opportunity to provide support, intervene early, prevent suicides, for men and women of all ages in all circumstances.
We should also be tackling those barriers to access at the point where people try to ‘reach out’ for support as well as developing more effective systems of us ‘reaching in’.
And we must continue to challenge the stigma and shame that prevents people from ‘seeking the right support’ as well as making sure the ‘right support’ is actually there.
Many people say they’re worried about urging their family, friends and colleagues to seek help because they’re not confident the help and support is actually there, or that they’ll get appropriate or effective support.
Support in ‘spotting the signs’ and pointing to guides and booklets and websites and online resources is fine as long as there’s actual support at the end of the search process.
Probably the most useful content in the National Strategy document, as it often is in any suicide prevention document, is lists like this of sources of information, services and initiatives to support people in need.
Publishing a national directory of services would have probably been more useful than the ‘strategy’ document we got!
Seriously though, we actually do have some great resources like, for example, the Hub of Hope (which is listed in the National Strategy document but could have been more prominent) where people can type in their postcode and find out what’s available in their area…
…and we should be doing more to make sure more people are aware of these excellent resources, to support and build capacity to support.
Virtually every week, I have a conversation with someone about the Hub of Hope as a start point in their search, and they weren’t previously aware, and it’s a revelation to them. We must all raise the general level of awareness and knowledge, and it should be another component of suicide education and mental health education in schools.
Also provide the content in the most useful way, eg by group, by issue or challenge being faced, by sector people work in, not just lists.
And try to make the lists of resources as comprehensive as possible.
A request I’ve had dozens of times in my mental health and suicide prevention research over the past 10 years is a system of referral and recommendation for all of the different sources and services available.
And another problem with top-down Government strategies that tend to mainly involve the bigger, more established charities, and a privileged few people with lived experience, they all run away from ideas like this, due to institutionalised conservatism, or put them in the ‘too hard basket’.
I’ve tried many times to work with government, at all levels, the NHS, other institutions and public services, and several charities…and none of them will touch the idea of a “referral and recommendation system” with a bargepole. They’re terrified of having any responsibility beyond ‘here’s a list’ — even then they’re terrified they’ve missed someone off the list! — and saying ‘this is good…we’d recommend this’.
Even when I’ve suggested a “TripAdvisor style approach with user recommendations and referrals”, the establishment looks the other way and goes back to its comfort zone, like identifying ‘priority groups’ or highlighting potential academic research projects or ONS analysis.
Interestingly, I mentioned the idea last month to the development team for the new iTalk mental health and suicide prevention app which has been designed initially for the Construction sector (where almost 10% of all suicides in England and Wales are to be found), and developed entirely with private funding from within the Construction sector, and they said immediately “we’ll develop that and build it into the app”!
This is the kind of ambition and practical innovation we need to be able to get the numbers of suicides on a downward trend, towards zero.
And watch this space for the roll out of the iTalk app:

Suicide Prevention in the Criminal Justice System
The content below is positive and hopeful, highlighting one area where there are lots of practical actions that can be taken to reduce suicides considerably — the justice system.
I recall one of my local suicide prevention partnerships having an overall target for reducing suicides as ‘10% in 5 years’ — the classic low ambition ‘10% reduction in 5 years’ problem manifesting itself once again — but having a reduction target for deaths in custody of 95%.
I asked them why their overall reduction target was so low but their target for reducing suicides in police custody was so high.
And the answer was very simple of course. They could think of the specific, practical actions they could take to reduce suicide deaths in custody, so aimed high. But they couldn’t think of practical actions to get the overall numbers down by more than 10% in 5 years, or they didn’t think they had the resources to get the overall suicide numbers down by more than 10%.
This is the psychology of suicide prevention which we need to understand and harness. Break it down into bite size chunks. Eat the elephant one bite at a time. Take each component part of the whole system and develop highly practical actions with those who would be responsible for taking those actions, in order to get the commitment that involvement brings.
It’s another reason why ‘The Priority Trap’ is so pernicious because the practical action plans are only encouraged and developed in a limited number of ‘priority areas’ for ‘priority groups’.

One significant concern I have with the above content is in relation to the line “Action to prevent suicide and self-harm is needed across the criminal justice system” — so far, so good — “in police custody, in prison services for those on remand or serving a sentence, in probation, and for all those on release”.
No mention at all of another huge source of distress and pain in the criminal justice system which is another driver of self-harm and suicide — its insensitive administrative incompetence!
I’ll highlight just two examples here.
Firstly, I have a family member who works in the courts trying to support witnesses as they give evidence. They of course provide emotional and psychological support independent of the case or circumstances, and don’t talk about the content of the court case to avoid any influence on the case.
What frequently happens is that it will be a really difficult case involving child sexual abuse or domestic violence, the trial has been delayed for months if not years, the witness finally gets a trial date, they make the physical arrangements for travel and accommodation, arrange time off work, and start preparing emotionally and psychologically…and then, a day or two before the due date, they’re told ‘the trial has been postponed’ and/or ‘it’s been moved to another court, in another jurisdiction’.
And the witness has to go through all this again, often twice or three times. There’s rarely an apology. There’s little or no support for these vulnerable people who’ve been further overloaded and distressed ‘by the system’.
Secondly, jurors, and I’ve experienced this personally.
Called for jury service as ‘ordinary, everyday citizens’, the jurors are thrust into some horrific cases, including child sexual abuse, domestic violence, exposure to harmful materials, and extreme cases like the Lucy Letby trial, listening to testimony week after week about the murder of babies.
In some jurisdictions, there’s some reasonable support for jurors as they prepare for and go through the trial, although not always, but there’s little or nothing after the trial.
Some of these experiences as a juror are life-changing and highly traumatising, and yet jurors are expected, at the end of the trial, to ‘go back to their normal lives’.
Their lives have just been changed forever. There’s no ‘normal’ any more. These people need access to counselling for the rest of their lives!
There should be mandatory access to counselling, as we’ve advocated for in our petition to parliament for a Suicide Prevention Act.
Autistic People
As with all of the ‘priority groups’ in this latest National Strategy, it’s great to see acknowledgement of the issues and potential steps that can be taken to reduce the number of suicides among autistic people, but the way the National Strategy process does this raises concerns.
Of course, there’s the problem of ‘The Priority Trap’, the biases, the ‘winners and losers’ approach that means autistic people are one of the ‘winners’ this time but there are many more non-prioritised groups who are ‘losers’ in the 2023 competition, including other neurodivergent groups. other than autistic people.
It’s interesting that this section begins with “Evidence suggests autistic people, including autistic children and young people, may be at a higher risk of dying by suicide compared with those who are not autistic”.
Note the cautious, non-committal language — “may be at a higher risk”.
At recent conferences I’ve attended, and in recent conversations with autistic people and advocates for autistic people, I’ve seen and heard suggestions that there’s a considerably higher suicide risk among autistic people and that at least 1 in 10 suicides could be autistic people.
Caution is understandable, not wanting to put out inaccurate data; and those involved in the National Strategy process tend to have a particular interest in data quality, with some harsh critics even going further, based on what they’ve observed, and saying ‘they’re more interested in data quality and accuracy than in actually reducing the number of suicides’!
But from a ‘dynamics of change’ perspective, until the scale of the problem is acknowledged, the Push factor for change, potential transformational change, is being constrained.
It’s also another example of data that’s been absent, ie there’s been a bias against autistic people in past National Strategies because the data and evidence wasn’t there, and wasn’t being collected, which then highlights the fact there are other biases still in place because of other gaps in the data and evidence.

Also, many of the advocates I’ve spoken with have been very keen to emphasise the danger of just focusing on autistic people and ‘seeing autistic people as the problem’ and then trying to provide autistic people with support and not seeing ‘society as the problem’ in terms of stigma and stereotypical attitudes, lack of understanding, bullying, prejudice, etc.
There’s a tendency for National Strategy processes like this to focus, first, on the ‘health issues’ of autistic people then, second, on the education needs of autistic people, only then widening out into other issues that autistic people have and need support for, with ‘changing society’s awareness, knowledge, understanding, attitudes and behaviours’ coming a long way down the list, if it appears at all, even though this might be the solution to a lot of the issues autistic people and their families face.
New Mothers. New Fathers?
It’s good to see a spotlight on ‘new mothers’ in this new National Strategy but the obvious next question is ‘what about new fathers?’.
Again, what seems to be happening here is another case of the ‘data and evidence bias’. The available data, and emerging evidence, suggests a heightened suicide risk among ‘new mothers’ (and pregnant women), and so this becomes a ‘priority group’ in the National Strategy — another ‘winner’ in the competition — whilst other groups are competition ‘losers’, including groups like menopausal women, new fathers, and perhaps some more specific groups such as parents who’ve experienced a miscarriage?

Financial Difficulty and Economic Adversity
Having a focus on “financial difficulty and economic adversity” is another welcome development, and getting the excellent charity, Money & Mental Health involved in the National Suicide Prevention Advisory Group is good:
But it’s disappointing it’s taken so long to have this focus. It seems to have taken a wider impact of the recent cost-of-living crisis on people who are working as well as those not working, to finally make this a ‘priority group’.
The National Strategy continues to give little confidence that the issues facing people losing their jobs are well understood with appropriate and effective support being forthcoming.
Experiences of losing a job — including unexpected and unwanted redundancy, unfair dismissal, an entire company unexpectedly going under — can be absolutely devastating.
And the lack of support and poor treatment for those losing their jobs, who also then can experience problems with housing, relationships, mobility, access to their children, deteriorating mental health…can be fatal.
It’s hard for people living in poverty, and people who experience long-term unemployment, although many of these people learn to cope and survive with levels of resilience most would find challenging to even imagine.
Often the highest suicide risk is among those who’ve never lived in poverty, never experienced unemployment before, never had to claim benefits, and certainly never had to rely on food banks.
Many of those who lose their jobs go from a relatively good salary or wage to ‘the breadline’ and, if they don’t have access to significant levels of savings, they’re in deep trouble.
Many of those who lose their jobs these days also lose the access they had to relatively good workplace wellbeing programmes, EAP, counselling, and find themselves in a position with no access to any such support.
Many cope for 2–3 months, eg if there’s a redundancy payout or ‘outplacement package’ which includes continued access to workplace wellbeing support for up to 3 months on exiting a business, or there are some savings to draw from, but then the suicide risk grows in months 4–5 if they don’t get another job.
The ‘financial difficulty and economic adversity’ content in this latest National Strategy doesn’t appear to cover the kinds of issues that quickly emerge in any qualitative or ethnographic research. This may be due to the tendency to focus on quantitative analysis of available data sets.
One of the least reassuring aspects of the National Strategy is the section on what DWP will do for its part in trying to reduce the numbers of suicides.
Just after I read this, I spoke at a suicide prevention conference where I parodied this proposal by saying “because of course when someone has lost their job and had to experience the pain and humiliation of dealing with DWP services, and have to fight to get benefits and support they should be seamlessly entitled to, and are shamed and stigmatised and treated as non-humans, and they’re made to jump through demeaning hoops, and they find themselves on a decline into hopelessness and entrapment, and feel like it’s no longer worth living…the first thing they’re going to do is call the DWP helpline and say they’re having thoughts of suicide”!
Yes, it is ridiculous isn’t it?! I’m afraid I tend to spiral into cynicism where DWP is concerned, even though I know some lovely individual human beings who work within their inhumane systems.
If DWP’s contribution to the National Strategy is largely waiting for people to call its helplines and disclose their suicidal thinking or planning, we’re not going to significantly reduce the estimated 500 suicides per year among unemployed (or underemployed) people.
Of course, I applaud efforts to have mandatory training for all front-line staff so they’re better able to spot signs and signpost. In terms of progress since the previous National Strategy, however, this does smack of ‘slightly more advanced lip service’.
Gambling and Suicide Prevention
When I lived and worked in Australia, I did a lot of research into gambling and the devastation it causes, and I helped to devise services and support, and also devise campaigns to try and encourage people to seek support, including one campaign that had to be pulled because it was “too successful” in getting take up of counselling!
In the course of my research, I saw and heard some horrific ‘stories’ about the devastating impact of gambling and how the betting companies create and sustain addiction, so this is an especially sensitive subject for me.
Once again, I welcome the focus on gambling-related suicide in the latest National Suicide Prevention Strategy, and I applaud the brilliant work of charities like Gambling with Lives to get this issue on the national agenda.
And, of course, I’m once again conscious of the ‘winners and losers’ model of the National Strategy process so as I see gambling-related suicides emerging as one of the ‘winners’ this time, largely due to the excellent advocacy of those who’ve been impacted, and I also think about the ‘losers’ in this national competition.
Once again, we read in this National Strategy document “There is increasing evidence…” around gambling-related suicide, despite the fact that the ‘evidence’ has been there for decades for anyone who wanted to look at it.
What they mean of course is their kind of evidence, ie some quantitative data brought to their attention showing a (potential) statistical correlation, possibly a causal relationship, between gambling addiction and suicides.
This is ‘evidence’ in the eyes of the suicide prevention establishment. Case studies of preventable suicides among people in the grip of gambling addiction back up the statistics, but are not sufficient to stimulate action.
Thankfully, this is starting to change but there’s still an emphasis on having ‘robust quantitative data’ and this is problematic when the absolute numbers might be ‘relatively small’ so not conducive to the number-crunching model, and where there’s not outrage at every single suicide death caused by betting companies feeding addiction, and when it needs an organised lobby group — a tiny ‘lobby group’ compared with the vast power and resources of the betting companies’ lobby — to get action.
It’s also disturbing that this opening sentence specifies “younger people”, ie “increasing evidence of the relationship between harmful gambling and suicide in younger people”. This problem is not just being experienced by younger people and it doesn’t take long to get out there and see that!
Hopefully, with advocates highlighting the issues around gambling-related suicides now having ‘a seat at the table’, these wider issues will be aired.
So, there are some signs and sources of hope, but such a long way to go when there’s such a power imbalance with the betting companies having so much power to do harm, and a weak response to calls for a total ban on betting companies’ advertising just like we have for smoking.
Also, once again, this is a highly political issue in many respects, eg the emphasis on ‘personal responsibility’ with the language being about ‘the problem gambler’ and getting ‘gambling addicts’ to ‘reach out’, and trying to help ‘people with a gambling problem’ and not focusing on the system and the betting companies that create and feed destructive addiction.
Domestic Abuse and Suicide Prevention
Domestic abuse is another example of an issue we’ve known much about for many years with informal and anecdotal information, plus some small-scale qualitative research, showing a relationship between domestic abuse and suicide (risk) but it’s taken some more robust quantitative research and analysis to get this issue to the ‘top table’ and into the National Strategy.
Well done to Tim Woodhouse and the Kent & Medway team who’ve brought forward the research and brought this issue to national attention.

It’s also another example of the dangers of ‘the Priority Trap’ and ‘The Top Down Trap’, ie ‘no (quant) data, no priority, no action’ and then the tendency to take an issue proven to be a particular driver of suicide or contributory factor in suicides in one area (Kent & Medway in this case) and advocating for every area to prioritise this, via ‘aligning with National Strategy priorities’ even though domestic abuse or domestic violence may not be a key issue or risk factor in other areas.

The fact that domestic abuse has now been given ‘priority status’ in the National Strategy means that it will now be given more prominence in more areas, and it will have more research and analysis around it, which will make it more likely to be a priority in more local suicide prevention strategies and plans…and so it goes on.
All good for tackling issues around domestic abuse, but not so good for all the other issues/groups not prioritised in the latest National Strategy.
Limiting Access to (Lethal) Means of Suicide
I recall a presentation by Professor Jane Pirkis of the University of Melbourne where she’d carried out a meta analysis of initiatives to reduce the numbers of suicides in various places around the world, and by far the most effective way of reducing the numbers of suicides was limiting access to the means of suicide, especially limiting access to lethal means.
It makes sense doesn’t it? Of course, we must have early intervention and upstream prevention to minimise the number of people even getting as far as making a suicide attempt but, sadly, people will get this far, and there’s much we can do to stop suicide plans and attempts becoming deaths.
So, it’s right that this appears in the National Strategy, although it could go much further.

In the media rounds when the National Strategy was released on 11 September, the Minister made several references to “emerging methods” and more specifically “places online where people can freely buy lethal drugs”.
This development is extremely worrying, of course, although there was an element here of the Minister ‘playing to the gallery’ because this was a high profile news story at the time the National Strategy was published.
When this topic was discussed in various forums after the National Strategy was released, it was also another example of the ‘top down mentality’ when there were suggestions that the Department for Education could inform schools about ‘emerging methods’ of suicide or self-harm risk.
In reality, many schools will be aware of these emerging methods and harmful sites long before DfE does! But, yes, everyone should share relevant information and guidance.
And this is a DfE remember that is yet to agree that we need suicide education in schools as part of the curriculum!
Maybe they should be committing to the principle, and developing specific proposals for covering online access to medication in the content.
I can hear the panicked cries already of ‘we wouldn’t want to put the idea into kids’ heads’, which is partly code for ‘we don’t want to be held liable’ , and which is not an ‘evidence-based reaction’ as, firstly, kids already know about this stuff anyway — what they don’t have is the education around it — and, secondly, there’s lots of research evidence that tells us you don’t make a healthy person suicidal by talking about suicide, you just help people who are suicidal, and need help, to get help.
Of course there are risks with ‘prompting experimentation’ but that’s another good reason why this needs proactive education to prevent suicides rather than a reactive response after a suicide when it’s too late.
Another long-standing issue which is now, thankfully, getting more attention is “frequently used locations” — what the public at large and media still often refer to as “suicide hotspots” but that language is regarded as unhelpful, possibly harmful, so we usually refer to ‘frequently used locations’ or some call them ‘high risk locations’.
I’ve had a conversation recently with the CEO of a high profile bridge and we talked about how we know what measures are needed to significantly reduce the numbers of suicides and we know how much these measures would cost but no-one is prepared to invest the necessary resources even though we know there’d be a high financial return on that investment as well as the reduction in human pain and suffering.
Unfortunately, ‘the system’ works against such suicide prevention activity, including the National Strategy process which, in its current form, is not going to generate the millions of pounds needed to make these types of high risk locations ‘suicide safer’.
This final paragraph above is another weak offering. “We would encourage those with a role in the planning system to consider…”?!
It doesn’t give us confidence, does it? Or much hope of action.
We should be demanding, and facilitating, a full-scale review of planning guidelines and the Building Regulations from a ‘suicide safer’ perspective!
And there’s also much scope for utilising ‘Tech for Good’ and ‘Digital Life Saving’ and ‘Tracking for Life’ technology to have better ‘digital-human systems’ working to prevent suicides in or near high risk locations.
Based on my own research and listening to people with lived experience of suicide, those reaching the point where they’re following through on their suicide plans have their smartphone with them and have it switched on. They often send a ‘final message’ or ‘do a final post’ on social media.
I’ve interviewed people who’ve lived through a suicide attempt — most of whom, by the way, don’t like the term ‘suicide survivor’, emphasising the importance of being sensitive to the language we use — and they’ve told me “I decided to put a post on [social media platform(s) of choice] and said to myself ‘if I don’t get a reply to this message, I’m going through with it’…”.
It was because of research like this that we developed the concept of ‘Digital Life Saving’ and why I took to the stage at TEDxSydney 2014 to urge everyone in the audience to develop initiatives to quickly identify people in danger from their publicly available social media posts to be able to instantly respond to them.
It’s sad there’s been so little progress in this field in the past 10 years. The main advances have been in improving search engines, improving advice via virtual assistants, and intercepts, including the fantastic browser-based intercept tool developed by Alice Hendy and her R;pple team:
So much more could be done. And rather than have positive, enthusiastic, creative support for these types of initiatives through processes like the National Strategy, there seems to be resistance, or perhaps just lack of awareness and education around what’s possible?
I noticed this line in the National Strategy: “The use of AI in predictive tools or in real-time conversations with individuals would not be appropriate”.
Why not? Why hold development back? Why slow the whole process of technological development and our capacity for suicide prevention to the pace that academics & government policymakers work at? Why not engage in partnerships right now to develop capabilities and learn as we go?
As it happens, ‘the use of predictive tools in real-time conversations’ is happening anyway so a Canute-style response from the National Strategy is not helpful and smacks of arrogance as well as possibly ignorance.
‘Tracking for Life’ apps have enormous potential, eg in tracking people — with their advance, informed permission — who’ve been discharged from hospital to help ensure they get home safely, including pinging (nominated contacts or emergency services) if they go near ‘frequently used locations’.
I’ve had little or no joy from ‘the establishment’ with all these ideas for reducing the numbers of suicides via ‘Tech for Good’ solutions but, in contrast, a very positive response from the oft-demonised ‘private sector’!
The new, privately-funded iTalk app, initially designed for, and funded by, the Construction sector, will incorporate some of these ‘Tracking for Life’ and ‘Digital Life Saving’ concepts and turn them into practical functionality. The iTalk team has the will and the way!
Bereavement Support for Suicide Prevention
This is another case of a positive development which needs to go further, deeper and wider; which needs to acknowledge inherent biases; and which illustrates the flaws in the National Strategy process as well as the benefits.
We’ve known for decades that loss and grief and trauma, and especially traumatic loss, has a massive adverse impact on people, which can increase their suicide risk. I personally experienced this after my dad died in 2010.
But formal, structured research around the impact of something like bereavement, especially quantitative research and analysis, is rare, so it’s struggled to get on the agenda for things like the National Strategy, because that’s the ‘system’ the National Strategy operates within…
…reacting to available data rather than being proactive; tending to react to quantitative data rather than qualitative insights; prompting, supporting and encouraging particular types of research into priority groups or priority actions or priority risk factors whilst discriminating against other groups/actions/factors; reacting to organised ‘lobby groups’, charities, advocates, campaigners putting forward a particular case, especially if they have ‘the right kind of data’, whilst neglecting other sources or factors causing or contributing to suicide.
Note that this section of the National Strategy begins with a very clear and specific statement “Evidence suggests family, friends and acquaintances who are bereaved by suicide may have a risk of dying by suicide that is up to 3 times higher than the general population”, with the usual get-out clause “may”.
Also note that no specific research sources are offered to support this statement. I’m not questioning the statement but it’s rather incongruous that those responsible for the National Strategy make such a fuss about having ‘data & evidence’ before anything goes into the National Strategy as one of its priorities, and yet no research references for this statement.

I’ve looked into this subject via the referenced publications and websites that quote statistics like this, which also often include a statement about those bereaved by suicide being more likely to die by suicide than those bereaved by other means, so-called ‘natural causes’.
There seems to be one piece of research that has fuelled acres of coverage:
https://bmjopen.bmj.com/content/6/1/e009948
It’s an interesting study, and it does indeed show that those in the sample were more likely to die by suicide if they’d been bereaved by suicide, and there’s no doubt that those who’ve lost someone to suicide should have ‘wrap around care & support’ and that ongoing support and future (health) interventions should take into account the family history of suicide, just as (health) professionals would ask about family history of cancer or diabetes.
However, please note that this is just one survey, carried out in 2010, among students and staff at UK universities, aged 18–40.
As any professional researcher will attest, we should exercise caution because it’s only one study, more than 10 years old, pre-COVID19, among a very specific audience and what’s effectively ‘a convenience sample’ of students and staff — as many academic research studies are as it’s easier and cheaper to ‘keep it on campus’ — and among a specific age range.
This study could be replicated among the same audience in 2023 — now including those losing people to COVID19 — or among a different group of 18–40 year olds, or a sample of 18–80 year olds…and get a different result.
Again let me be clear, I’m not doubting that those bereaved by suicide are more likely to die by suicide themselves, and I want to see the fullest possible support for those bereaved by suicide.
But I’m highlighting bias/discrimination creeping in to these processes.
Some people and organisations advocating for being a priority in the National Strategy will be told they don’t have a strong case, not enough data or evidence, and they need to go away to gather more data and evidence.
Meanwhile, another case is being accepted on the strength of one or two research studies that are often quoted without highlighting their limitations, combined with having someone on the Advisory Group putting this particular case, often from ‘case studies’ rather than more robust quantitative data, in contradiction to practice for other groups or issues.
Most importantly, loss and grief is not a competition. We shouldn’t be setting out to argue that bereavement by suicide is a special case. It’s just become a special case because of ‘the bubble effect’.
Those working in suicide prevention, those bereaved by suicide, and those responsible for putting the National Suicide Prevention Strategy together consider themselves as working ‘in suicide prevention’ and their primary interest is suicide & suicide prevention, not bereavement more widely or other specific forms of bereavement, eg by cancer, stroke, COVID19, etc.
When I did my counselling training and qualifications, and I did an Advanced Study Major in Loss & Grief, and I carried out research into loss, grief, trauma, and traumatic loss, I found that people bereaved by any means were at a higher suicide risk, and the group with the highest suicide risk after bereavement was older men losing their lifelong partner where the risks were high regardless of how their wife had died.
So when I read in the National Strategy “there is widespread recognition that improving bereavement support is an important goal in its own right, and bereavement is a risk factor for suicide among family, friends and acquaintances”, I think ‘yes, important to get that support around people bereaved by suicide…and important to get that support around all people who are bereaved’.
As Chukes Maxwell says “there’s no hierarchy in suffering”, and as I’ve found myself saying a lot recently “bereavement is not a competition”.
We mustn’t assume that a person might or might not be struggling after a bereavement, or might be struggling more or less than someone else, just as we mustn’t make assumptions about or discriminate against anyone in suicidal crisis, just try to have personalised safety plans for everyone.
We should be equally concerned about everyone at risk or in danger.
It’s part of the ‘at risk group’ mentality that makes people go looking first for a ‘group at risk’ then ‘individuals in danger’ within the group they’ve prioritised, which means two forms of bias or discrimination — first against other groups and everyone in those groups then, second, against everyone in their prioritised group they’ve created a hierarchy or risk profile for.
An alternative approach is to focus, first and foremost, on individuals in danger not groups at risk, and try to support everyone via a co-ordinated approach where ‘everyone is a priority for someone’, and not fall into ‘The Priority Trap’ and the other traps that come with beginning and ending your processes with “there are limited resources…there’s only so much we can do…we have to set priorities and allocate scarce resources…not everyone can be a priority…” which is effectively saying “there have to be winners and losers”.
It doesn’t have to be like this!
Suicide Can Affect Anyone and Everyone Can Help Prevent Suicides
I’ve commented on this earlier in this dissertation, so just a quick recap.
The key message to get across to everyone is a two part message. Firstly, “suicide can affect anyone”. Secondly “everyone can help prevent suicides”.
These two statements have been well researched and road-tested.
They get attention. They have impact, They’re inclusive, in terms of being embraced by almost everyone. And they don’t push people away.
So, we should be using such language in our advocacy, in our campaigns, in all our communications around suicide and suicide prevention, and in the National Suicide Prevention Strategy.
Another ‘no brainer’!
Too often though, we see language that isn’t so inclusive or ‘positive impact assured’, even though those using it are trying to achieve the same result.
Two key examples of this are “suicide is everyone’s business” and, especially, “suicide is everyone’s responsibility”.
Most people don’t think suicide is their business or their responsibility. When they hear these messages, they can be puzzled, offended, distressed, annoyed…especially being told it’s their responsibility which sounds very preachy and finger-wagging, so it has the opposite effect to that intended.
All of the measures set out below can be communicated to the public without us needing to explicitly use language like ‘everyone’s business’ or ‘everyone’s responsibility’.
No point pushing people away with such language, especially when we can pull them in to the conversation with the more inclusive and engaging “Anyone can be affected by suicide, and everyone can help prevent suicides”.

The Role of Employers, Sectors, Professions, and Communities at Work
In our report ‘Moving Towards a Zero Suicide Society’, we emphasise the role that ‘the workplace’ has in suicide prevention and this includes industries, sectors, and professions as well as individual employers and individual workplaces or — to reflect the flexible way people work these days plus changing thinking about the nature of workplaces — what we would call ‘communities at work’ because that’s what they should be ideally to help support each other, including when someone is struggling or in crisis, including when a whole team or business is struggling or in crisis.
In the National Suicide Prevention Strategy, the emphasis is on individual employers for whatever reason, with a note below “ONS will publish analysis in 2023 to provide updated information about suicide rates across different occupations, which will inform further evidence-based action”.

This is consistent, of course, with the Government’s National Strategy process which is centred on quantitative data and evidence, analysis of patterns and trends, identifying ‘risk groups’, setting priorities, and focusing attention on the agreed ‘priority groups’ or ‘risk factors’…
…creating and sustaining that competition for priority status with winners and losers in the competition the Government’s National Strategy process has constructed.
Despite the fact we already know that almost 1 in 10 suicides are among people in the Construction sector, there’s no explicit mention of this in the National Suicide Prevention Strategy or any strategy or plan to work with the Construction sector to get these numbers down. Why is this?
Call to Action?!
Most of the people I’ve spoken with who work in suicide prevention and who’ve read the National Strategy document have said they’re not inspired by it, and it doesn’t come across as an engaging ‘call to action’. I’d agree.
So it was interesting to get to this section at the very end of the document using those very words.
For a call to action to be more than just words, to energise people and get them wanting to take action, it must engage their hearts and minds and inspire them with hope and with confidence, and with a belief that ‘this is going to make a difference’.
This National Strategy fails to do that, partly due to its very limited Engagement & Involvement of key stakeholders, especially the wider community of people with lived or living experiences of suicide; partly due to the uninspiring content and language; partly due to the lack of a compelling vision so lack of the important Pull factor in The 3 Key Dynamics of Change model; and partly due to the lack of a Push factor…
…ie, the absence of a narrative which says, prominently and frequently, “this level of (5-6,000+) deaths we’ve had in England/UK for the past 15 years is totally unacceptable, and largely preventable, so we’re going to aim to get these numbers on a long-term downward trend, towards zero”.
In a so-called civilised society, we should expect nothing less.
In the Zero Suicide Society vision we’ve mapped out in our report ‘Moving Towards a Zero Suicide Society’, we do expect nothing less, and we set out the practical actions that will get us there.

It’s also interesting to read this line at the end “we have published a summary of actions alongside the strategy, setting out clearly where action will happen, by who and when”.
Most of those I’ve sought feedback from so far don’t think this is clearly the case. Indeed, they say they’ve been told by DHSC and members of the National Suicide Prevention Strategy Advisory Group that “developing action plans is actually the next phase”.
Furthermore, I’ve personally been told by people directly involved in the National Strategy process that “we’re working on action plans which will have targets”. I look forward to seeing these and doing some maths!
Last but not least, when I read a document, I’m always conscious that it’s easy to comment on what’s there but it’s just as important to see what’s not there; and, throughout this critique, I’ve tried to highlight the gaps.
In this final Call to Action section, it refers to bringing together “national and local government, the health service and the VCSE sectors”.
What about ‘the private sector’? What about commercial sectors and organisations who are a big part of the problem and potentially a big part of the solution — from reducing suicides among their workforce to providing the technological innovation that could be a breakthrough in suicide prevention?
It’s often the case that ‘the private sector’ is excluded from processes like the National Strategy, eg due to the prejudice of ‘public good, private bad’, due to the ‘seats around the table with representatives’ mentality that then finds it hard to justify having just 1 or 2 ‘representatives’ from something as broad and diverse and little understood as ‘the private sector’, and/or due to the hierarchical culture that believes ‘we regulate the private sector, we’re not equal partners with them’.
But we are equal partners when it comes to suicide prevention. To get the numbers of suicides down, towards zero, we have to be all be equal partners in a truly collaborative partnership around our common goals.
Mandatory Requirement: the Zero Suicide in Healthcare Framework
When I was working in suicide prevention in Australia, in the period 2013–2019, I worked closely with Sue Murray who was the highly successful and popular CEO of Suicide Prevention Australia who then founded the Zero Suicide Institute of Australasia.
Sue & I were worried about the lack of progress in getting the suicide numbers down, and decided to focus more on the growing ‘Zero Suicide’ movement around the world, with cases of considerable reductions in the numbers of suicides where the ‘Zero Suicide in Healthcare’ framework had been applied — 50%, 60%, 70%+ reductions.
I took a broader community perspective. Sue zeroed in (pun intended!) on the ‘Zero Suicide in Healthcare’ model, initially developed in the US, in Detroit, and developed it for Australia’s health system:
https://lifeinmind.org.au/suicide-prevention/collaborations/zero-suicide-healthcare-framework
When we ask people in our network, ie people who work in suicide prevention and people with lived experience who, like me and Steve Phillip, have made it their life mission to get the numbers of suicides on a downward trend towards zero, “what will get those numbers down?”…
…we regularly hear “well, here’s another ‘no brainer’ — mandatory roll out of the proven evidence-based ‘Zero Suicide in Healthcare Framework’ across the NHS and all healthcare organisations, so they can all individually work towards zero suicides in their Trust or healthcare organisation and we can collectively ‘move towards zero’ across the whole system and across the whole country”.
Btw, I’m dedicating that previous ‘no brainer’ summary to Rob Shipley who is a tireless advocate for the ‘Zero Suicide in Healthcare’ framework and is currently implementing it in his Trust.
But I’ve scoured the National Suicide Prevention Strategy for England, 2023–2028, I’ve read every word and re-read every word (I know, I’m a policy nerd, and among the 0.1% of the population who’ve read the document end-to-end!) and I can’t see anywhere “Mandatory Implementation of the Zero Suicide in Healthcare Framework”.
Why?
I’ve asked a few individuals privately and raised this question in some public forums. The responses I get tend to fall into two camps. One is people who don’t seem to actually know what the ‘Zero Suicide in Healthcare’ framework is, which is rather worrying if they’re responsible for developing the National Strategy. The other camp is those who clearly do know what the framework is but have chosen to reject it, which is odd.
In amongst the ignorance and prejudice, there are lots of ill-informed comments like “we’re not going to get to zero suicides, there’ll always be suicides”. In fact, the ‘Zero Suicide in Healthcare’ community of thinkers and practitioners make it clear that the Zero Suicide model & framework is not just a numerical target and that it’s rare to be able to eliminate suicides in any sizeable system, but that it’s a philosophy and a framework for aiming high and getting the suicide numbers down as far as possible and keeping them down at the lowest possible level. Hence ‘a no brainer’!
Those who do know what the ‘Zero Suicide in Healthcare’ philosophy and framework are gave me some better informed responses — albeit tending to be out-of-date — including concern about whether the NHS is in a good enough place at the moment to absorb it, whether staff would embrace it given the pressures on them, and whether the necessary resources to start the process would be made available.
As a fully signed-up member of the ‘this is a no brainer’ club, I’d counter each of those objections, including the fact that it pays for itself, staff will embrace it with the right leadership, and it could well be exactly what the NHS needs right now because the ‘Zero Suicide in Healthcare’ model is not only a good practice approach for ‘continuous, systemic, action learning’ that can bring down the suicide numbers, it’s a transferable process with transferable benefits.
Postscript: A Curious Message from the Government
When the National Suicide Prevention Strategy for England for 2023–2028 was published on 11 September 2023, there was much disappointment in its apparent lack of ambition and some concern about the lack of a target for reducing the numbers of suicides. For some, it felt like ‘giving up’!
When the Minister, Maria Caulfield MP, did the media rounds on the day of release, she was trying to claim ambition where there was little or no evidence of ambition, as well as trying to claim considerable progress since 2012 when there was little evidence of progress, and no decline at all in the annual number of suicides over that period.
When questioned about the lack of a reduction target, she waffled and obfuscated and looked like a Minister not on top of her brief.
A very curious thing then happened on 27 September.
As someone who, in addition to launching our own petition, has signed previous petitions to parliament for measures to reduce suicides, I received this same email message twice from the Government, once because I’d signed the 3 Dads Walking petition for suicide education to be in the school curriculum, the one which got 170,000 signatures…

…and one for The LEARN Network’s petition for a statutory duty of care for higher education students, which got 128,000 signatures.
Now, when I signed those petitions, I remember it said there’d be a formal written response to the petition proposals from the Government after 10,000 signatures, which I got, on both occasions, and I recall thinking how uninspiring those responses were.
I don’t recall signing up for communication from the Government about its National Suicide Prevention Strategy.
I can see how someone, in good faith, might think it relevant and might think we’d want to know that a new National Strategy had been published, despite the fact there were no further commitments in the document on either of these petition proposals.
It’s actually possible that the Government here is in breach of its GDPR duties because it does not have the explicit informed consent of those who, like me, signed these petitions and agreed only to receiving updates about these petitions and these petition proposals.
I then read the email message from the Government:

I couldn’t believe my eyes when I got to the bit that says “The strategy aims to half the number of suicides over the next five years”.
After failing to commit to a reduction target when the NSPS 2023–2028 was first published on 11 September, and having tried to defend its decision to not have a reduction target in the Strategy, was the Government now saying it was aiming to reduce the suicide numbers by 50%?
It was unlikely they’d done a U-turn of course and, with no new money allocated to the new Strategy, unlikely that the Government would be able to achieve a 50% reduction in the suicide numbers.
So was this cock-up or conspiracy?
Was it an innocent ‘administrative error’ or a devious way of trying to send out what the Government thought would be a positive message about the Government’s new Suicide Prevention Strategy to the 200,000+ people who’d signed these petitions?
I suspected it probably was more likely to be cock-up than conspiracy but, as well as posting publicly about this…
…I sent a private message to 100 people (working in suicide prevention), including 4 people I knew were involved in the National Strategy process.
Interestingly, I had a response from one person saying “Obviously cock up — the fact it says ‘half’ the number of suicides rather than ‘halve’ the number tells us it’s an administrative error”, and yet 80% of the responses I received said “conspiracy”, which is probably a reflection of the lack of trust people have in this current Government.
I initially brushed it off as still probably an ‘administrative error’ but had lingering concerns about the fact that any message had been sent, the unauthorised nature of the message, and the potential harm from misinformation or spin.
Then, as I now finish off writing this piece more than 2 months after these email messages were sent, I’m thinking “surely, if it was an administrative error and it got one of the most important pieces of content in the entire Strategy fundamentally wrong, there’d be an apology and a correction issued?”.
But, of course, there’s been no apology, and no correction.
Sadly, incompetence, if that’s what it was, doesn’t breed confidence.
And, if was a deliberate political act, that’s giving us even less confidence that this Government is remotely interested in minimising suicides.
Time to round-up and round off…and do what we do at The Jordan Legacy and across our Zero Suicide Society community…finish on a note of hope!
Moving Towards a Zero Suicide Society — What We Must Do!
In Jan 2023, The Jordan Legacy defined a ‘Zero Suicide Society’ as “a society that is willing and able to do all it can to prevent all preventable suicides”.
By having everyday conversations around this definition, as well as carrying out semi-structured action research around this definition, we’ve been able to flesh out in detail what a ‘Zero Suicide Society’ looks like and the practical actions that will get us there.
We’ve applied, indeed embraced, the 3 Key Dynamics of Change with the huge Pull effect from our highly motivating vision, our ongoing efforts to Involve — along with accepting that we need to do way more here — and the big Push effect from continuously communicating about the unacceptably & needlessly high numbers of suicides…and all the reasons why we need to have high ambition and not settle for low ambition as the latest NSPS has.
As a final thought to take away with us, perhaps we should add that in a Zero Suicide Society we would all be willing and able to do all we can to Involve, to Pull, and to Push towards zero.
As a ‘change coach’, I was taught that anything not taking us towards achieving our goal is potentially a barrier to us achieving our goal.
As highlighted in this critique, there’s much in this National Suicide Prevention Strategy 2023–2028 that is not taking us towards our goal of getting the suicide numbers on a downward trend, towards zero, and which is clearly creating barriers to us achieving that goal.
Several of those who were involved in the process of devising the NSPS (who some would describe as ‘the privileged few’) told me that the discussions were very calm, considered, respectful, polite…and those with lived or living experiences of suicide who were invited often had a reputation for being calm, considered, respectful, polite…and everyone worked together very harmoniously with a great sense of ‘team spirit’.
It all sounds really nice doesn’t it? And I always try my best to be a calm, considered, respectful, polite, harmonious team player wherever I think we’re a team where everyone is fully committed to a shared goal of getting the suicide numbers on a downward trend, towards zero, and demonstrating they have the capability to do so.
If, however, this approach isn’t getting the numbers of suicides down, towards zero, and appears to be leading to ‘satisficing’, devising and agreeing on low ambition strategies and plans, and public communications that play down the problem, overclaim on progress, use language that lessens the impact of our 3 Key Dynamics of Change, and seems to be leading to the ‘capture’ syndrome where those with high ambition get into bed with those who have low ambition and get ‘infected with low ambition’, perhaps we need to be a little less calm, polite or ‘groupthink harmonious’?
Maybe we need to show more passion? Maybe get a bit more angry about the lack of ambition, lack of progress, and apparent attempts (unintended consequences of a cosy approach?) to talk up any evidence of progress whilst talking down the size and scale of the problem we’re trying to solve?
We should always remain respectful and considered, and not make it personal as everyone is trying to help in their own way — even if there are unintended barriers & harms — but not be too passive, especially as there’s so much we can to get the suicide numbers down, towards zero.
My own approach in these situations is to say at the beginning of a meeting, workshop or forum “I’ll be a calm, considered, respectful, polite contributor to the discussion…but if, at any point, I see low ambition, overclaiming on progress, misrepresentation of data to fulfil personal or organisational agendas, unhelpful hype, or political spin, or anything that is a systemic barrier to us getting the numbers of suicides on a downward trend, towards zero, you might find me getting angry”!
The warning upfront helps people to see that your (controlled) anger is coming from a good place!
Finally, maybe to get the suicide numbers on that downward trend, towards zero, we need to take inspiration from Howard Beale (although the ironic twist here is that Beale was ultimately being controlled by the faceless power brokers in charge of the Network!), remind ourselves — as citizens, taxpayers, and human beings — that 5–6,000 preventable suicide deaths every year is totally unacceptable, and we should shout from the rooftops “I’m as mad as hell, and I’m not going to take this anymore”?!
[ps — I know some people don’t approve of the word ‘mad’ but, as someone living with mental illness, I’m owning it, and think it’s use in terms of being ‘mad’ at the lack of progress in getting the suicide numbers down is highly appropriate!]
Paul Vittles is a researcher, consultant, coach and counsellor who now specialises in suicide prevention and mental health.
Paul has lived with mental illness for 20 years, he’s experienced suicide loss multiple times — the first as far back as 1980, the most recent August 2020 — and has worked professionally in suicide prevention for more than 10 years in Australia and the UK.
Paul’s work in the UK these days is primarily with The Jordan Legacy, where he’s ‘Chief Facilitator, Zero Suicide Society Transformation Programme’.
Paul’s mission is to see the Zero Suicide Society Transformation Programme implemented, to move towards a Zero Suicide Society, and to get the UK suicide numbers on a downward trend, towards zero.
If you want to support the work The Jordan Legacy does, you can donate via the website or you can make a donation specifically to support The Jordan Legacy’s action research project via this Just Giving page:
